

Meniscus injuries within the knee are a common occurrence. So why is it that what we do during meniscus repair rehabilitation is so outdated?
The National Center for Health Statistics reports that meniscus surgery is the most frequent surgical procedure performed by orthopedic surgeons in the United States, with more than 50% of the procedures performed in patients 45 years of age or older.
Despite this high occurrence, many inconsistencies continue to exist in the rehabilitation of a patient following meniscus repair surgery, particularly involving the rate of weightbearing and range of motion.
I’m still shocked by this and wanted to discuss the recent research that is lending to a more progressive approach to return people safely back to their prior level of function.
Rehabilitation Follow Meniscus Repair

Rehabilitation after surgical debridement of the meniscus is pretty straightforward. We return the patient’s range of motion, strength and function per their symptoms and let pain and swelling guide the rehab process (a very general guide but one often employed by many rehabilitation specialists).
However, when the meniscus is actually repaired and not just debrided, there are other factors to consider. When a meniscus is repaired, the tear is approximated using stitches to allow the tear to heal.
Rehabilitation following a meniscus repair has to be more conservative, however, despite research saying otherwise, there are still many rehabilitation protocols floating around the orthopaedic and sports medicine world that recommend limiting weight-bearing and range of motion after a meniscal repair. We continue to ignore the literature because of fear that the ‘stress’ on the meniscus with walking and range of motion may be too high.
Unfortunately, many of these commonly used protocols are from the 1990s. (Click here for the updated rehabilitation protocols we currently use.)
So if we’re going to talk 90’s protocols, take a look at these studies from way back when from Shelbourne and Barber that showed excellent results in patients undergoing a combined ACL-meniscus repair procedure and utilizing no limitations in weightbearing or range of motion, similar to a protocol for an isolated ACL reconstruction.
Recent studies from VanderHave and Lind on isolated meniscus repairs have shown similar results using an “aggressive” program of immediate weightbearing compared to a more conservative approach.
I certainly wouldn’t consider these “aggressive” programs, they simply used immediate weightbearing and range of motion.
Again, these studies show meniscal repair outcomes are no different while using restricted weightbearing and range of motion versus an “aggressive” protocol of immediate weight-bearing and unlimited range of motion.
Early Weightbearing After Meniscus Repair

But what about the exact mechanisms that many are still fearful of allowing early in the process, like early walking and range of motion? Won’t that put the repair in a position to fail?
We typically immobilize people in full extension during weightbearing, locked in a brace for 4-6 weeks after meniscal repair surgery.
So, if immobilized in extension, why do we limit weightbearing?
During weightbearing, compressive forces are loaded across the menisci. These tensile forces create ‘hoop stresses’, which expand the menisci in extension. These hoop stresses are thought to be helping the healing process in many tears by approximating the tissue.
Furthermore, the compressive loads applied while weightbearing in full extension following a vertical, longitudinal repair or bucket-handle repair have been shown to reduce the meniscus and stabilize the tear, as noted by Rodeo and more recently by McCulloch.
Range of Motion After Meniscus Repair
What about early range of motion?
There is very limited literature on the influences of range of motion on meniscal movement. Thompson showed that during flexion, the posterior excursion of the medial meniscus was 5.1 mm, while that of the lateral meniscus was 11.2 mm.
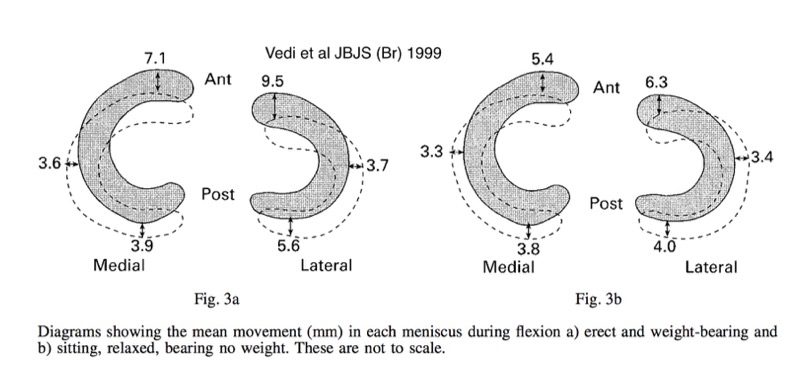
Looking at meniscal movement as the knee flexes in weightbearing and non-weightbearing you can see there’s less motion, although I really don’t think we know how much motion is detrimental. The motion has been shown to help improve blood flow to the area. This is huge and may aid in the healing process!
What Do We Recommend?
Anecdotally, I can say we have handled meniscal repairs to allow weightbearing and range of motion to tolerance for many years. Some of the top orthopedic surgeons in the world that I have worked with currently handle a meniscal repair the same as an ACL reconstruction with a meniscal repair .
For an isolated meniscal repair, I prefer the knee continue to be immobilized in full extension for 4-6 weeks but allowed full weightbearing immediately (if a longitudinal repair). For complex repairs, I would recommend limiting weightbearing to partial but understand that the hoop stresses could aid in healing and are arguably helpful and necessary. For both cases, I would recommend passive range of motion to tolerance.
Trust me, I respect the healing meniscus and continually monitor patients as I progress their range of motion and weight-bearing activities. Things like new joint line pain along the site of the repair, new swelling or a change in pain patterns, and even clicking (although most people have this) are all signs that I may want to further assess and modify my progression.
Based on this, I continue to stand by my rehab guidelines of full, pain-free passive range of motion and immediate weightbearing after a vertical longitudinal meniscal repair. The literature is screaming this same thing at us but we continue to ignore their calls and revert to the ’90s!
What do the surgeons that you work with recommend? Are any of them still recommending rehab guidelines based on outdated research? Comment below and let me know, I want to hear what the rest of the country is seeing!
Learn How We Evaluate and Treat the Knee

For those interested in learning more about how Lenny and I evaluate and treat the knee, we have an amazingly comprehensive course that covers everything you need to know to master the knee. Our detailed examination process, all our treatment progressions, and detailed information on nonoperative and postoperative treatment of ACL, patellofemoral, meniscus, articular cartilage, osteoarthritis injuries, and so much more.



