Shoulder instability is a common injury encountered in physical therapy. But there are many different types of shoulder instability.
Would you treat a high school baseball player that feels like their shoulder is loose when throwing the same as a 35 year old that fell on ice onto an outstretched arm and dislocated their shoulder? They both have “shoulder instability,” right?
There exists a wide range of symptomatic shoulder instabilities from subtle recurrent subluxations to traumatic dislocations. Nonoperative rehabilitation is commonly utilized for shoulder instability to regain previous functional activities through specific strengthening exercises, dynamic stabilization drills, neuromuscular training, proprioception drills, scapular muscle strengthening program and a gradual return to their desired activities.
But to truly understand how to successfully treat shoulder instability, there are several key factors that you must consider.
Key Factors When Designing Shoulder Instability Rehabilitation Programs
Because there are so many different variations of shoulder instability, it is extremely important to understand several factors that will impact the rehabilitation program. This will allow us to individualize shoulder instability rehabilitation programs and enhance recovery.
There are 6 main factors that I consider when designing my rehabilitation programs for nonoperative shoulder instability rehabilitation. I’m going to cover each in detail.
Factor #1 – Mechanism and Chronicity of Shoulder Instability
The first factor to consider in the rehabilitation of a patient with shoulder instability is the mechanism and chronicity of the injury. There are two different types of instability that can be classified as:
- Acute, traumatic instability
- Chronic, atraumatic instability
Pathological shoulder instability may result from an acute, traumatic event or chronic, recurrent instability. The goal of the rehabilitation program may vary greatly based on the onset and mechanism of injury.
Following a traumatic subluxation or dislocation, the patient typically presents with significant tissue trauma, pain and apprehension. The patient who has sustained a dislocation often exhibits more pain due to muscle spasm than a patient who has subluxed their shoulder. Furthermore, a first time episode of dislocation is generally more painful than the repeat event.
Here’s a great example of a traumatic dislocation. Note the amount of pain the athlete is in as they walk off the field with the shoulder still dislocated.
Rehabilitation will be progressed based on the patient’s symptoms with emphasis on early controlled range of motion, reduction of muscle spasms and guarding and relief of pain. But the main goal is to allow the shoulder capsule to heal.
The primary traumatic dislocation is most often treated conservatively with immobilization in a sling and early controlled passive range of motion (ROM) exercises especially with first time dislocations.
The incidence of recurrent dislocation ranges from 17-96% with a mean of 67% in patient populations between the ages of 21-30 years old. Therefore, the rehabilitation program should progress cautiously in young athletic individuals. It should be noted that Hovelius has demonstrated that the rate of recurrent dislocations is based on the patient’s age and not affected by the length of post-injury immobilization. Individuals between the ages of 19 and 29 years are the most likely to experience multiple episodes of instability. Hovelius also noted patients in their 20’s exhibited a recurrence rate of 60% whereas patients in their 30’s to 40’s had less than a 20% recurrence rate. In adolescents, the recurrence rate is as high as 92% and 100% with an open physes.
Conversely, a patient presenting with atraumatic instability often presents with a history of repetitive injuries and symptomatic complaints. Often the patient does not complain of a single instability episode but rather a feeling of shoulder laxity or an inability to perform specific tasks.
They often times also have the ability to move their shoulder into excessive motion.

Rehabilitation for this patient should focus on early proprioception training, dynamic stabilization drills, neuromuscular control, scapular muscle exercises and muscle strengthening exercises to enhance dynamic stability due to the unique characteristic of excessive capsular laxity and capsular redundancy in this type of patient.
Chronic subluxations, as seen in the atraumatic, unstable shoulder may be treated more aggressively due to the lack of acute tissue damage and less muscular guarding and inflammation. Rotator cuff and periscapular strengthening activities should be initiated while ROM exercises are progressed. Caution is placed on avoiding excessive stretching of the joint capsule through aggressive ROM activities.
Remember, in these patients, the primary need is stability, not mobility.
The goal is to enhance strength, proprioception, dynamic stability and neuromuscular control especially in the specific points of motion or direction which results in instability complaints.
Factor #2 – Degree of Shoulder Instability
The second factor is the degree of instability present in the patient and its effect on their function.
Varying degrees of shoulder instability exist such as a subtle subluxation or gross instability. The term shoulder subluxation refers to the complete separation of the articular surfaces with spontaneous reduction.
Conversely, a dislocation is a complete separation of the articular surfaces and requires a specific movement or manual reduction to relocate the joint. This will result in underlying capsular tissue trauma. Thus, with shoulder dislocations the degree of trauma to the glenohumeral joint’s soft tissue is much more extensive.
In the situation of an acute traumatic dislocation, the anterior capsule may be avulsed off the glenoid. This is called a Bankart lesion, and the posterior capsule may be stretched, allowing the humeral head to dislocate. This has been referred to as the “circle stability concept.”
Speer has reported that in order for a shoulder dislocation to occur, a Bankart lesion must be present and also soft tissue trauma must be present on both sides of the glenohumeral joint capsule.
The rate of progression will vary based upon the degree of instability and persistence of symptoms. For example, a patient with mild subluxations and muscle guarding may initially tolerate strengthening exercises and neuromuscular control drills more than a patient with a significant amount of muscular guarding.
Factor #3 – Concomitant Pathology
The third factor involves considering other tissues that may have been affected and the premorbid status of the tissue.
As we previously discussed, disruption of the capsulolabral complex from the glenoid commonly occurs during a traumatic injury resulting in an anterior Bankart lesion. But other tissues may also be involved.
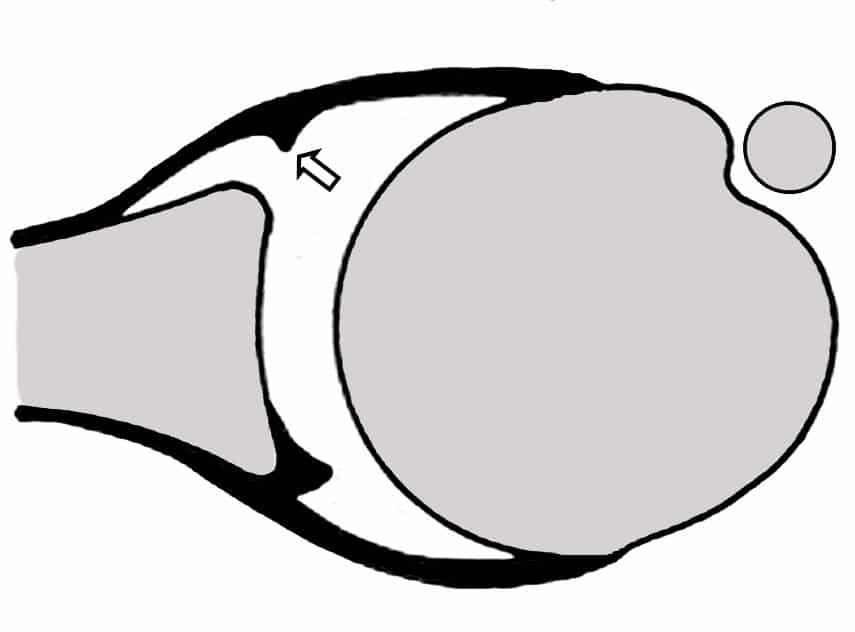
Often osseous lesions may be present such as a concomitant Hill Sach’s lesion caused by an impaction of the posterolateral aspect of the humeral head as it compresses against the anterior glenoid rim during relocation.
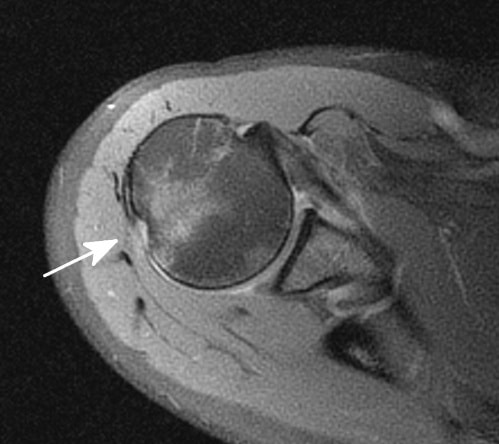
This has been reported in up to 80% of dislocations. Conversely, a reverse Hill Sach’s lesion may be present on the anterior aspect of the humeral head due to a posterior dislocation. Similarly, the glenoid can also sustain a boney lesion.
The more boney involvement, the greater amount of instability that is often present.
Occasionally, a bone bruise may be present in individuals who have sustained a shoulder dislocation as well as pathology to the rotator cuff. In rare cases of extreme trauma, the brachial plexus may become involved as well. Other common injuries in the unstable shoulder may involve the superior labrum (SLAP lesion) such as a type V SLAP lesion characterized by a Bankart lesion of the anterior capsule extending into the anterior superior labrum. These concomitant lesions will affect the rehabilitation significantly in order to protect the healing tissue.
Factor # 4 – Direction of Shoulder Instability
The next factor to consider is the direction of shoulder instability present. The three most common forms include anterior, posterior and multidirectional.
Anterior shoulder instability is the most common traumatic type of instability seen in the general orthopedic population. It has been reported that this type of instability represents approximately 95% of all traumatic shoulder instabilities. However, the incidence of posterior instabilities appears to be dependent on the patient population. For example, in professional or collegiate football, the incidence of posterior shoulder instability appears higher than the general population. This is especially true in linemen. Often, these posterior instability patients require surgery as Mair reported 75% required surgical stabilization.
Following a traumatic event in which the humeral head is forced into extremes of abduction and external rotation, or horizontal abduction, the glenolabral complex and capsule may become detached from the glenoid rim resulting in anterior instability, or a Bankart lesion as discussed above.
Conversely, rarely will a patient with atraumatic instability due to capsular redundancy dislocate their shoulder. These individuals are more likely to repeatedly sublux the joint without complete separation of the humerus from the glenoid rim.
Posterior shoulder instability occurs less frequently, only accounting for less than 5% of traumatic shoulder dislocations.
This type of instability is often seen following a traumatic event such as falling onto an outstretched hand or from a pushing mechanism. However, patients with significant atraumatic laxity may complain of posterior instability especially with shoulder elevation, horizontal adduction and excessive internal rotation due to the strain placed on the posterior capsule in these positions.
Multidirectional instability (MDI) can be identified as shoulder instability in more than one plane of motion. Patients with MDI have a congenital predisposition and exhibit ligamentous laxity due to excessive collagen elasticity of the capsule.
One of the most simple tests you can perform to assess MDI is the sulcus sign.

I would consider an inferior displacement of greater than 8-10mm during the sulcus maneuver with the arm adducted to the side as significant hypermobility, thus suggesting significant congenital laxity. You can see this pretty good in this photo, the sulcus is clearly larger than my finger width.
Due to the atraumatic mechanism and lack of acute tissue damage with MDI, range of motion is often normal to excessive.
Patients with recurrent shoulder instability due to MDI generally have weakness in the rotator cuff, deltoid and scapular stabilizers with poor dynamic stabilization and inadequate static stabilizers. Initially, the focus is on maximizing dynamic stability, scapula positioning, proprioception and improving neuromuscular control in mid range of motion.
Also, rehabilitation should focus on improving the efficiency and effectiveness of glenohumeral joint force couples through co-contraction exercises, rhythmic stabilization and neuromuscular control drills. Isotonic strengthening exercises for the rotator cuff, deltoid and scapular muscles are also emphasized to enhance dynamic stability.
Factor #5 – Neuromuscular Control
The fifth factor to consider is the patient’s level of neuromuscular control, particularly at end range.
Injury with resultant insufficient neuromuscular control could result in deleterious effects to the patient. As a result, the humeral head may not center itself within the glenoid, thereby compromising the surrounding static stabilizers. The patient with poor neuromuscular control may exhibit excessive humeral head migration with the potential for injury, an inflammatory response, and reflexive inhibition of the dynamic stabilizers.
Several authors have reported that neuromuscular control of the glenohumeral joint may be negatively affected by joint instability.
Lephart compared the ability to detect passive motion and the ability to reproduce joint positions in normal, unstable and surgically repaired shoulders. The authors reported a significant decrease in proprioception and kinesthesia in the shoulders with instability when compared to both normal shoulders and shoulders undergoing surgical stabilization procedures.
Smith and Brunoli reported a significant decrease in proprioception following a shoulder dislocation.
Blasier reported that individuals with significant capsular laxity exhibited a decrease in proprioception compared to patients with normal laxity.
Zuckerman noted that proprioception is affected by the patient’s age with older subjects exhibiting diminished proprioception than a comparably younger population.
Thus, the patient presenting with traumatic or acquired instability may present with poor neuromuscular control that must be addressed.
Factor # 6 – Pre-injury Activity Level
The final factor to consider in the nonoperative rehabilitation of the unstable shoulder is the arm dominance and the desired activity level of the patient.
If the patient frequently performs an overhead motion or sporting activities such as a tennis, volleyball or a throwing sport, then the rehabilitation program should include sport specific dynamic stabilization exercises, neuromuscular control drills and plyometric exercises in the overhead position once full, pain free motion and adequate strength has been achieved.
Patients whose functional demands involve below shoulder level activities will follow a progressive exercise program to return full ROM and strength. The success rates of patients returning to overhead sports after a traumatic dislocation of their dominant arm are often low, but possible.
Arm dominance can also significantly influence the successful outcome. The recurrence rates of instabilities vary based on age, activity level and arm dominance. In athletes involved in collision sports, the recurrence rates have been reported between 86-94%.
Keys to Shoulder Instability Rehabilitation
To summarize, nonoperative rehabilitation of shoulder instability has many subtle variations. To simplify my thought process, I always think of these 6 key factors before I decide what I want to focus on for each person.
Learn How I Evaluate and Treat the Shoulder
Want to learn exactly how I rehabilitate shoulder instability?
I have a whole lesson on this as part of my comprehensive online program on the Evidence Based Evaluation and Treatment of the Shoulder. If you want to learn exactly how I evaluate and treat the shoulder, including shoulder instability, this course is for you. You’ll be an expert on shoulders!