What is the best special test for a SLAP tear? There are many options all with varying efficacy, however, without a proper understanding of the different types of SLAP tears and mechanisms of injury, it’s difficult to select the best special test for SLAP tears.
Remember, SLAP tears are just one type of shoulder labral tears, as the superior labrum is just a portion of the glenoid labrum.
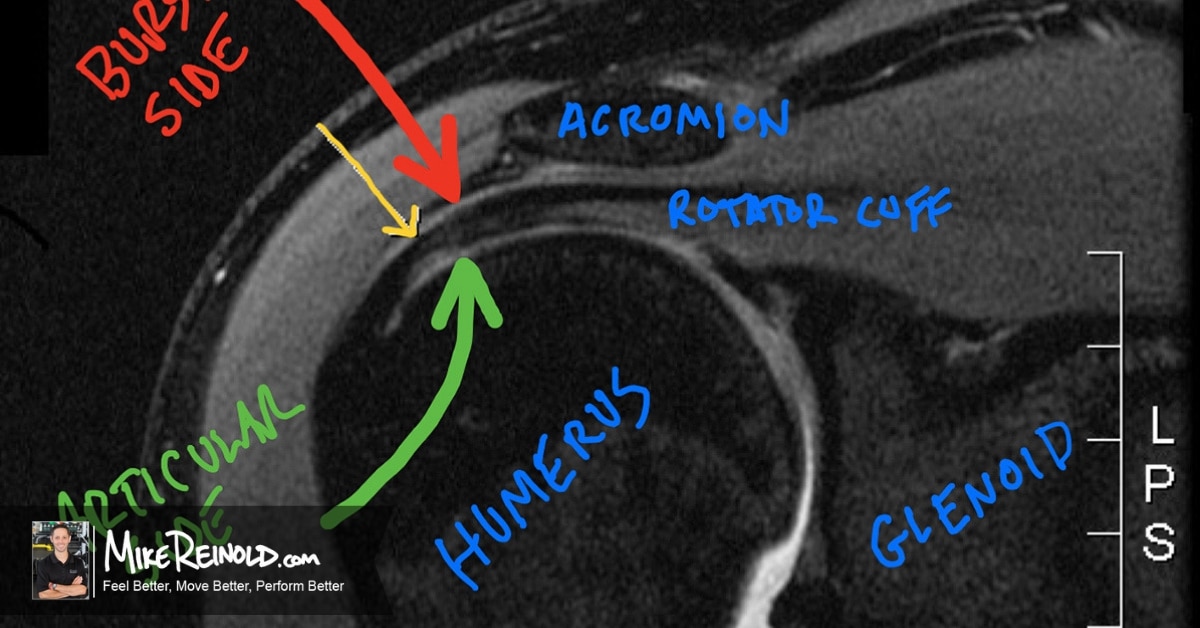
Clinical examination to detect SLAP lesions is often difficult because of the common presence of concomitant pathology in patients presenting with this type of condition. Andrews has shown that 45% of patients (and 73% of baseball pitchers) with superior labral lesions have concomitant partial thickness tears of the supraspinatus portion of the rotator cuff. Mileski and Snyder reported that 29% of their patients with SLAP lesions exhibited partial thickness rotator cuff tears, 11% complete rotator cuff tears, and 22% Bankart lesions of the anterior glenoid.
The clinician should keep in mind that while labral pathologies frequently present as repetitive overuse conditions, such as those commonly seen in overhead athletics, the patient may also describe a single traumatic event such as a fall onto the outstretched arm or an episode of sudden traction, or a blow to the shoulder. This is an extremely important differentiation you need to make when selecting which tests you should perform.
A wide variety of potentially useful special test maneuvers have been described to help determine the presence of labral pathology. Let’s review some of them now.
- Part 1: Classification of SLAP Lesions
- Part 2: Mechanism of SLAP injuries
- Part 3: Special Tests for SLAP Lesions (You are here)
- Part 4: How to Choose Which SLAP Test to Perform
Special Tests for a SLAP Tear
There are literally dozens of special tests for SLAP tears of the shoulder. I am going to share some of the most popular SLAP tests.
Active Compression Test
 The active compression test is used to evaluate labral lesions and acromioclavicular joint injuries. This could be the most commonly performed test, especially in orthopedic surgeons. I am not sure why, though, I do not think it is the best.
The active compression test is used to evaluate labral lesions and acromioclavicular joint injuries. This could be the most commonly performed test, especially in orthopedic surgeons. I am not sure why, though, I do not think it is the best.
The shoulder is placed into approximately 90 degrees of elevation and 30 degrees of horizontal adduction across the midline of the body. Resistance is applied, using an isometric hold, in this position with both full shoulder internal and external rotation (altering humeral rotation
against the glenoid in the process). A positive test for labral involvement is when pain is elicited when testing with the shoulder in internal rotation and forearm in pronation (thumb pointing toward the floor). Symptoms are typically decreased when tested in the externally rotated position or the pain is localized at the acromioclavicular (AC) joint.
O’Brien et al found this maneuver to be 100% sensitive and 95% specific as it relates to assessing the presence of labral pathology. These results are outstanding, maybe too outstanding. Pain provocation using this test is common, challenging the validity of the results. In my experience, the presence of deep and diffuse glenohumeral joint pain is most indicative of the presence of a SLAP lesion. Pain localized in the AC joint or in the posterior rotator cuff is not specific for the presence of a SLAP lesion. The posterior shoulder symptoms are indicative of provocative strain on the rotator cuff musculature when the shoulder is placed in this position.
The challenging part of this test is that many patients will be symptomatic from overloading their rotator cuff in this disadvantageous position.
- Sensitivity: 47-100%, Specificity: 31-99%, PPV: 10-94%, NPV: 45-100% (a lot of variability between various authors)
Biceps Load Test
 involves placing the shoulder in 90 degrees of abduction and maximally externally rotated. At maximal external rotation and with the forearm in a supinated position, the patient is instructed to perform a biceps contraction
involves placing the shoulder in 90 degrees of abduction and maximally externally rotated. At maximal external rotation and with the forearm in a supinated position, the patient is instructed to perform a biceps contraction- Sensitivity: 91%, Specificity: 97%, PPV: 83%, NPV: 98% for Biceps Load I; Sensitivity: 90%, Specificity: 97%, PPV: 92%, NPV: 96% for Biceps Load II
Compression Rotation Test
 The compression-rotation test is performed with the patient in the supine position. The glenohumeral joint is manually compressed through the long axis of the humerus while the humerus is passively rotated back and forth in an attempt to trap the labrum within the joint. This is typically performed in a variety of small and large circles while providing joint compression when performing this maneuver, in an attempt to grind the labrum between the glenoid and the humeral head. Furthermore, the examiner may attempt to detect anterosuperior labral lesions by placing the arm in a horizontally abducted position while providing an anterosuperior directed force. In contrast, the examiner may also horizontally adduct the humerus and provide a posterosuperiorly directed force when performing this test. I think of this test as “exploring” the joint for a torn labrum. It is hit or miss for me.
The compression-rotation test is performed with the patient in the supine position. The glenohumeral joint is manually compressed through the long axis of the humerus while the humerus is passively rotated back and forth in an attempt to trap the labrum within the joint. This is typically performed in a variety of small and large circles while providing joint compression when performing this maneuver, in an attempt to grind the labrum between the glenoid and the humeral head. Furthermore, the examiner may attempt to detect anterosuperior labral lesions by placing the arm in a horizontally abducted position while providing an anterosuperior directed force. In contrast, the examiner may also horizontally adduct the humerus and provide a posterosuperiorly directed force when performing this test. I think of this test as “exploring” the joint for a torn labrum. It is hit or miss for me.
- Sensitivity: 24%, Specificity: 76%, PPV: 90%, NPV: 9%
Dynamic Speed’s Test
 The Speed’s biceps tension test has been found to accurately reproduce pain in instances of SLAP lesions. I have personally not seen this to be true very often.
The Speed’s biceps tension test has been found to accurately reproduce pain in instances of SLAP lesions. I have personally not seen this to be true very often.
It is performed by resisting downwardly applied pressure to the arm when the shoulder is positioned in 90 degrees of forward elevation with the elbow extended and forearm supinated. Clinically, we also perform a new test for SLAP lesions.
Kevin Wilk and I developed a variation of the original Speed’s test, which we refer to as the “Dynamic Speed’s Test.” (I came up with the name, what do you think?) During this maneuver, the examiner provides resistance against both shoulder elevation and elbow flexion simultaneously as the patient elevates the arm overhead. Deep pain within the shoulder is typically produced with shoulder elevation above 90 degrees if this test is positive for labral pathology.
Anecdotally, we have found this maneuver to be more sensitive than the originally described static Speed’s test in detecting SLAP lesions, particularly in the overhead athlete. To me, it seems like you only get symptoms with greater degrees of elevation, making the original Speed’s Test less sensitive in my hands.
- Sensitivity: 90%, Specificity: 14%, PPV: 23%, NPV: 83% for the Speed’s test
Clunk Test and Crank Tests
 The clunk test is performed with the patient supine. The examiner places one hand on the posterior aspect of the glenohumeral joint while the other grasps the bicondylar aspect of the humerus at the elbow. The examiner’s proximal hand provides an anterior translation of the humeral head while simultaneously rotating the humerus externally with the hand holding the elbow. The mechanism of this test is similar to that of a McMurray’s test of the knee menisci, where the examiner is attempting to trap the torn labrum between the glenoid and the humeral head. A positive test is produced by the presence of a clunk or grinding sound and is indicative of a labral tear.
The clunk test is performed with the patient supine. The examiner places one hand on the posterior aspect of the glenohumeral joint while the other grasps the bicondylar aspect of the humerus at the elbow. The examiner’s proximal hand provides an anterior translation of the humeral head while simultaneously rotating the humerus externally with the hand holding the elbow. The mechanism of this test is similar to that of a McMurray’s test of the knee menisci, where the examiner is attempting to trap the torn labrum between the glenoid and the humeral head. A positive test is produced by the presence of a clunk or grinding sound and is indicative of a labral tear.
The crank test can be performed with the patient either sitting or supine. The shoulder is elevated to 160 degrees in the plane of the scapula. An axial load is then applied by the examiner while the humerus is internally and externally rotated in this position. A positive test typically elicits pain with external rotation. Symptomatic clicking or grinding may also be present during this maneuver. These tests seem to do well with finding a bucket-handle tear of from a Type III or Type IV SLAP lesion more than anything else for me.
- Sensitivity: 39-91%, Specificity: 56-93%, PPV: 41-94%, NPV: 29-90%
2 New(er) Special Tests for SLAP Lesions
In addition to the classic SLAP tests that have been described, there are two additional tests that gained popularity more recently.
I wanted to share a video that I have on YouTube that demonstrates these two tests. These were actually published in a paper I wrote in JOSPT a few years ago, but I have modified them a little and wanted to share. These two tests are both excellent at detecting peel-back SLAP lesions, specifically in overhead throwing athletes, but are useful for any population. I share these two tests because I know that there is a lot of confusion regarding the “best” test. These may not be them, but in my hands, both have been extremely helpful and, more importantly, accurate.
Pronated Load SLAP Test
The first test is the “Pronated Load Test,” it is performed in the supine position with the shoulder abducted to 90° and externally rotated. However, the forearm is in a fully pronated position to increase tension on the biceps and subsequently the labral attachment. When maximal external rotation is achieved, the patient is instructed to perform a resisted isometric contraction of the biceps to simulate the peel-back mechanism. This test combines the active bicipital contraction of the biceps load test with the passive external rotation in the pronated position, which elongates the biceps. A positive test is indicated by discomfort within the shoulder.
Resisted Supination External Rotation SLAP Test
The second test was described by Myers in AJSM, called the “Resisted Supination External Rotation Test.” Dr. Myers was a fellow at ASMI and a good friend of mine, he really wanted to call this the SUPER test (for SUPination ER) but I was one of many that advised him against this for obvious reasons!
During this test, the patient is positioned in 90° of shoulder abduction, and 65-70° of elbow flexion and the forearm in a neutral position. The examiner resists against a maximal supination effort while passively externally rotating the shoulder. Myers noted that this test simulates the peel-back mechanism of SLAP injuries by placing maximal tension on the long head of the biceps by supinating.
Myers’ study of 40 patients revealed that this test had better sensitivity (82.8%), specificity (81.8%), positive predictive value (PPV) (92.3%), negative predictive value (NPV) (64.3%), and diagnostic accuracy (82.5%) compared to the crank test and extremely popular O’Brien’s or active compression test. A positive test is indicated by discomfort within the shoulder.
When Do You Perform These Tests?
Now that you know a bunch of special tests for SLAP tears, the real key is understanding “when” to pick each test. In my mind, they all are slightly different and may even be better at detecting different types of SLAP lesions. I have an Inner Circle webinar that discusses this and shows you my clinical algorithm on how and why I perform special tests to diagnose a SLAP tear:
Learn Exactly How I Evaluate and Treat the Shoulder
 If you want to learn even more about the shoulder, my online course will teach you exactly how I evaluate and treat the shoulder. It is packed with tons of educational content that will help you master the shoulder, including detailed information on the clinical examination and treatment of SLAP tears.
If you want to learn even more about the shoulder, my online course will teach you exactly how I evaluate and treat the shoulder. It is packed with tons of educational content that will help you master the shoulder, including detailed information on the clinical examination and treatment of SLAP tears.