
If you’ve been following baseball at any level over the past several years, you already know that injuries to baseball pitchers continue to rise.
UCL injuries and Tommy John surgeries are happening at younger ages and at higher rates than ever before. Over 39% of current MLB pitchers have undergone UCL reconstruction at some point in their careers. But more importantly, we are seeing injuries in younger patients.
The majority of UCL injuries now occur in high school and college players.
Surgical techniques have improved dramatically. We now have traditional UCL reconstruction (Tommy John surgery), the newer UCL repair with internal brace augmentation, and a hybrid reconstruction combining the traditional reconstruction with the internal brace. Each has a different recovery timeline.
But regardless of how good the surgery gets, none of it matters if we don’t get the return-to-sport process right.
An important and often under-appreciated component of any rehabilitation program is the interval throwing program — the structured process of gradually returning a pitcher back to full competitive throwing.
I’ve recently published my interval throwing programs for baseball players in two articles in IJSPT. I’m happy to send them to you (see the end of this article).
But let me explain a little bit about them first!
What Is a Baseball Interval Throwing Program?
An interval throwing program (ITP) is a stepwise protocol designed to progressively return a pitcher to full competitive throwing after injury or surgery.
We often say that the body adapts to the stress applied to it. But we can’t forget that it also adapts when stress is removed!
After months off following surgery, a pitcher’s healing tissues need to be gradually reloaded before they can handle the demands of pitching in games.
The classic structure of an ITP involves a flat-ground progression — starting at short distances like 30-45 feet and progressively moving out to 120 feet or beyond — followed by a mound progression that works up through bullpen sessions and eventually live game situations.
The variables that drive workload are distance, volume (throw count), frequency (how often you throw), and intensity (how hard you throw).
The workload progression must be gradual and consistent. Too fast, and you overwhelm healing tissue. Too slow, and you fail to build the tissue tolerance needed to compete.
Quantifying Workload: The Concept of Acute:Chronic Workload Ratio
One of the most important advances in rehabilitation and sports science over the past decade has been the introduction of workload management concepts from people like Tim Gabbett.
The idea is straightforward but powerful: track how much work an athlete is doing right now (the “acute” workload, calculated as a 7-day rolling average) relative to what they’ve been doing over the past four weeks (the “chronic” workload, a 28-day rolling average).
That acute:chronic workload ratio, or ACWR, tells you whether an athlete is doing too much, too little, or just the right amount relative to what their body is prepared for. Research across multiple sports has consistently shown that injury risk increases when the ACWR exceeds 1.3 or falls below 0.7. The sweet spot is somewhere between those values.
Here the classic image from Tim Gabbett’s research:

In baseball specifically, a study by Mehta tracked 18 high school pitchers for an entire season. Pitchers whose ACWR exceeded 1.27 were 14.9 times more likely to suffer a throwing-related injury. That’s a pretty big increase in injury risk.
When designing our new interval throwing programs, we wanted to make sure we were using appropriate workloads.
But the first question we set out to answer: are the interval throwing programs we’ve been using actually keeping pitchers within this safe ACWR range?
The answer, it turns out, was not great.
The Problem with Traditional Interval Throwing Programs
I want to be upfront about something: the most widely used interval throwing program in baseball over the past 25 years came from a paper I published back in 2002 with Kevin Wilk and many other colleagues.
I’ve been proud of that work — it’s been used successfully by thousands of players and referenced in numerous outcome studies.
It works; that has been proven.
But I’ve also been quietly building and using a better version for many years, and honestly, the old program was starting to show its age.
Traditional ITPs, including ours, were based on clinical experience and expert opinion rather than biomechanical data. We were doing our best with the tools and knowledge we had at the time. But over the past 20 years, our understanding of the biomechanics of throwing has advanced significantly.
We now understand how elbow varus torque changes when performing an ITP. We also have workload management frameworks. We have data from hundreds of thousands of throws.
There were also some practical issues with the old format that I didn’t love, especially after working within professional baseball and seeing how a healthy pitcher trains.
Traditional programs prescribed throws in sets and repetitions with rest breaks between sets — a format more familiar to a physical therapy clinic than a baseball field.
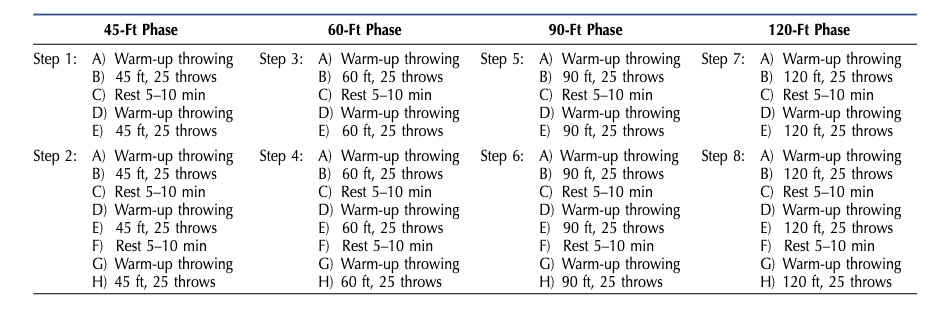
Modern players don’t train that way. I always thought players felt more like “patients” than “athletes,” which created buy-in problems and, frankly, didn’t reflect how pitchers actually prepare.
I wanted to build something that felt like baseball so that when an injured player starts throwing, they feel more like an athlete than a patient.
Building the ITP Workload Model
The first step in building better programs was to establish an accurate, objective way to quantify the workload of every throw. My colleague, Brittany Dowling, used elbow torque data from a database of 238,611 throws from healthy NCAA Division I college pitchers. From that data, they created a second-order polynomial regression equation that predicts peak elbow varus torque based entirely on throwing distance.
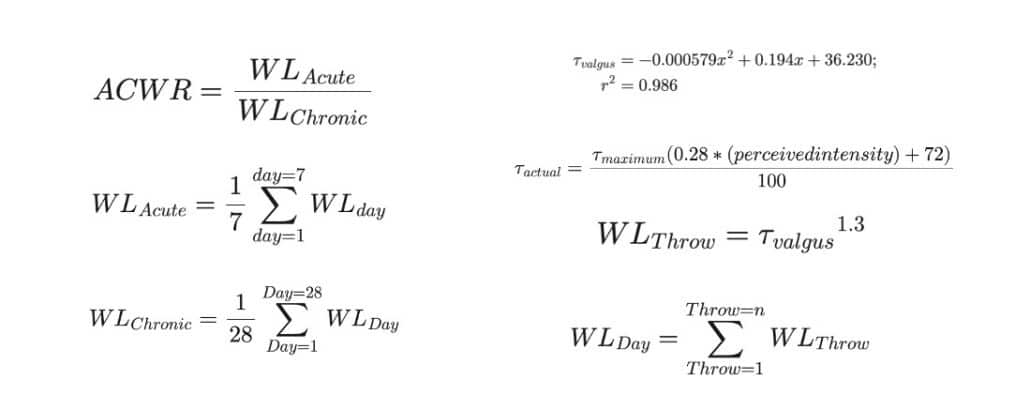
The key insight from this model is that torque increases meaningfully as throwing distance increases from 30 feet to about 120 feet, after which it plateaus. Throwing at 120 feet produces elbow varus torque roughly equivalent to pitching off a mound.

This is similar to many other published biomechanical models. Here’s a graph from Dias in IJSPT that shows similar data and also how the torque increased on a mound progression as intensity increases:
By the way… this is why most long toss programs stop at 120 feet. Once you throw to 120 feet, your healing tissue is technically prepared for the stress of the mound. Could you throw further? Sure, but it will slow the program down.
Our programs use distance to dictate intensity. There are other ways to measure intensity, including ratings of perceived exertion and velocity measured with radar, but we use distance because it is the most reliable and accessible proxy for actual biomechanical stress on the elbow (more on this below).
Once Dowling established the model, they used it to reverse-engineer what existing programs were actually doing to a pitcher’s arm. Their study analyzed three prominent ITPs widely used at major sports medicine institutions affiliated with Major League Baseball.
The results were close, but not perfect.
- Program A (136-day schedule): The ACWR spiked above or below the safe range of 0.7–1.3 a total of 19 times. Final chronic workload: 15.0.
- Program B (157-day schedule): The ACWR spiked out of the safe range 21 times. Final chronic workload: 13.0.
- Program C (187-day schedule): The ACWR spiked out of the safe range 23 times. Final chronic workload: 8.4.
As you can see, they were all over the place for frequency, chronic workload, and ACWR.
The three most popular interval throwing programs in baseball rehabilitation were exposing pitchers to suboptimal spikes in workload between 19 and 23 times over the course of a single program.
Not once or twice, nearly two dozen times.
The same study then used computational modeling to design a new, optimized ITP model, reverse-engineered to maintain a steady ACWR within the safe range throughout the entire program. The result was a 146-day schedule with a final chronic workload of 14.2 and zero ACWR spikes outside the safe range after the first 28 days of throwing.
It proved that building a model program this way was possible. Now, I wanted to make it look and feel like a program familiar to modern baseball pitchers.
Building the New Interval Throwing Program
Using the workload model from Dowling et al. as our scientific foundation, we set out to build an interval throwing program that was both biomechanically optimized and practically applicable to the modern baseball pitcher.
This led to the publication of our 7-month program designed primarily for long-term rehabilitation following significant surgeries like Tommy John reconstruction, SLAP repairs, labral lesions, and rotator cuff tears.
It is very humbling to me that we won two research awards for this one study – the Major League Baseball Research and the International Journal of Sports Physical Therapy Research of the Year Awards.

The program’s structure was deliberately designed to mirror how healthy baseball players actually train.
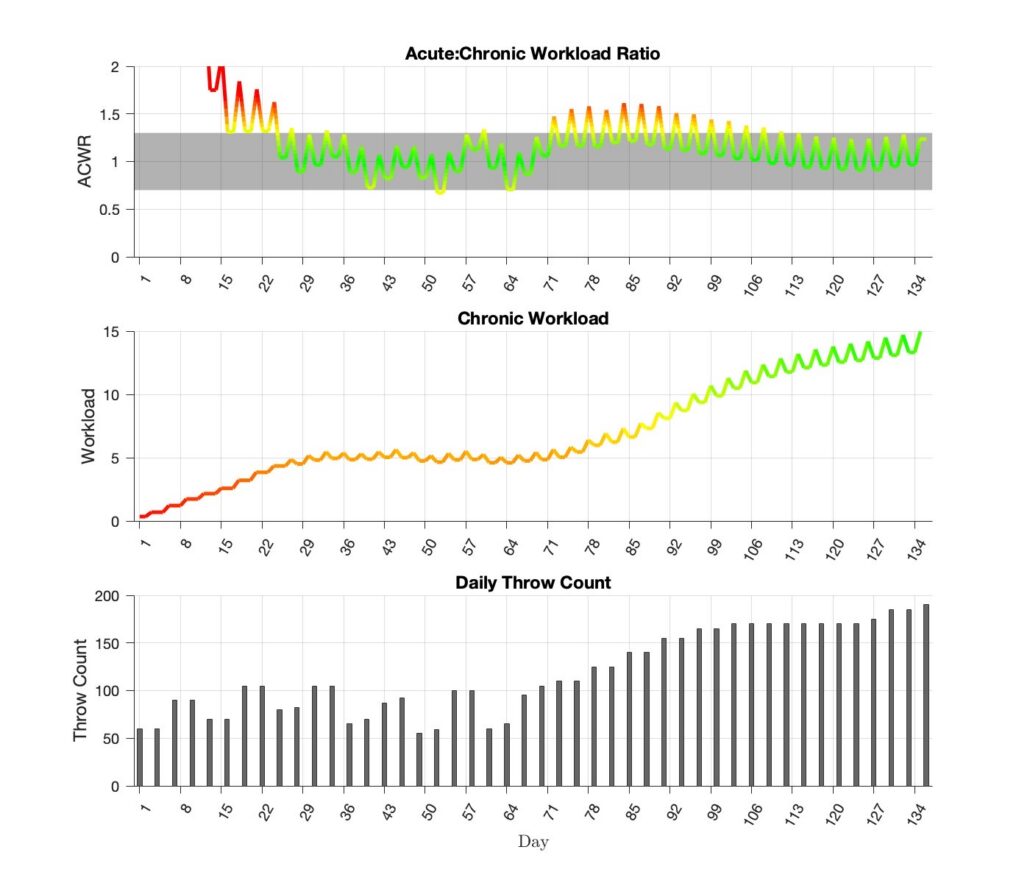
Instead of repeated sets and reps with mandated rest breaks, every day of the program had a sequential progression of intensity and volume of a specific throwing prescription.
Each day was different and precisely structured. Compare this format to the one above. It’s much more gradual and progressive, while removing any unnecessary structure.

The flat-ground progression begins at 30 feet — short and easy enough for even the most post-operative arm to handle with confidence — and progresses gradually out to 120 feet.
Long-toss throwing incorporates a step-and-shuffle approach with an arc trajectory, allowing distance to drive intensity naturally without requiring pitchers to consciously “throw at 50% effort” (which is, by the way, nearly impossible to do accurately and leads to inconsistent loading). Pulldowns are added toward the end of the long-toss phase to increase intensity as the arm approaches mound readiness.
Strategically placed deload weeks at Weeks 7, 14, 22, and 29 give the arm a deliberate break from the linear progression, reducing the risk of accumulated fatigue and supporting recovery.
These deload weeks required careful programming to ensure ACWR didn’t drop below the safe range or spike when returning to throw, but getting them right was worth it.
Players consistently report feeling so much better after a deload week.
The mound progression begins at Week 16 with a return to flat-ground pitching mechanics before moving to the mound. Fastball intensity use percentage of perceived exertion, starting at 50% and increasing incrementally to 75%, 90%, and finally 100%. Using perceived exertion on the mound is more valid than using it during a long-toss progression. Secondary pitches are reintroduced in stages, and the later weeks of the program include live at-bat sessions with limited pitch counts.
Here’s what the 7-month program looks like in regard to chronic workload and ACWR:
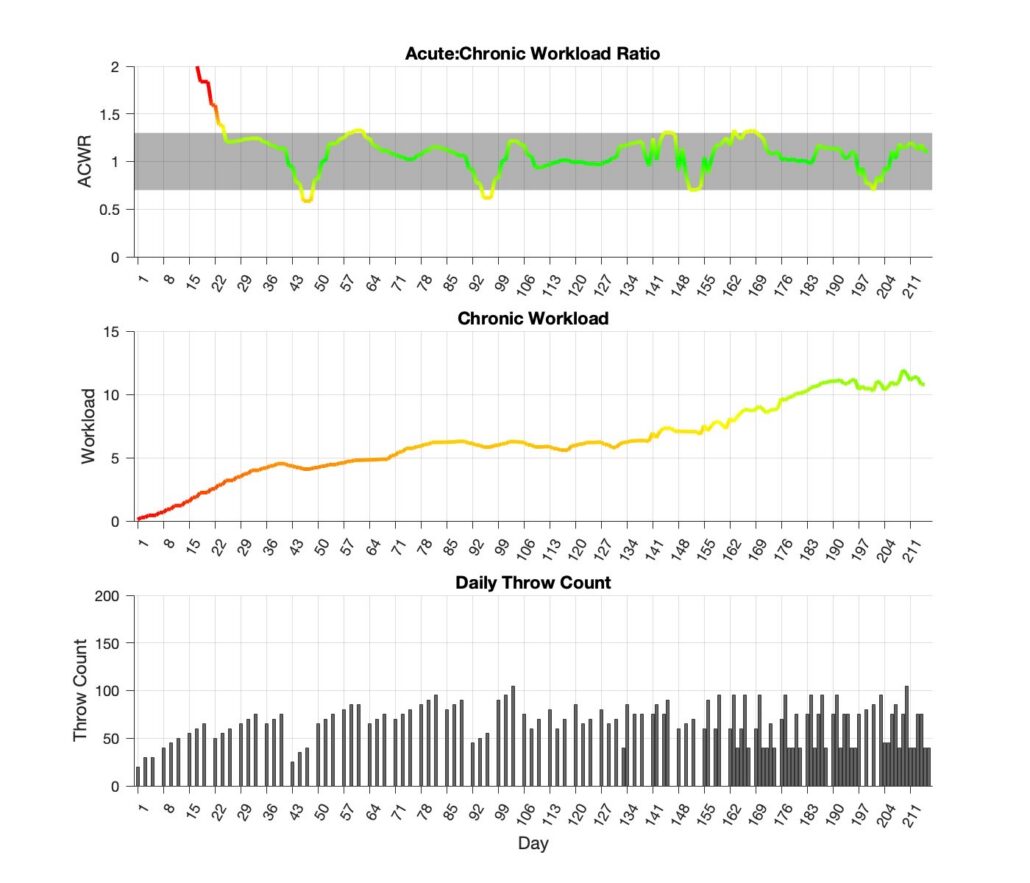
How Does it Compare to the Old Program?
When we ran the workload analysis on our updated 7-month program and compared it directly to our original 2002 program, the differences were significant:
- Original ITP: 136-day schedule, final chronic workload of 15.0, ACWR outside the safe range for 18% of the program, with a peak ACWR of 1.61 (24% higher than the upper optimal limit).
- Updated ITP: 217-day schedule, final chronic workload of 10.8, ACWR outside the optimal range for only 9% of the program, with a peak ACWR of 1.33, just barely above.
That’s a major improvement in both the acute workload management and the final chronic workload.
Here’s the part that really matters to me clinically: the original program finished with a chronic workload of 15.0, which is equivalent to mid-season workload levels for active pitchers.
When pitchers come back from Tommy John and feel exhausted and underperform in their first year back, this might be a big reason why. We were returning them to competition at the same workload as someone who’d been pitching all season.
The updated program builds to a chronic workload of 10.8. High enough to prepare the arm for competition, but with room left to continue building naturally as the pitcher re-enters the competitive season.
This gradual approach should allow athletes to be more competitive in their first year back and reduce the common experience of feeling “gassed” and not returning to form until their second season post-surgery.
Expanding the Framework: Multiple Duration Programs for Every Injury
The 7-month program is ideal for the most significant surgeries, but the reality of baseball injuries is much more varied. A player with a mild UCL sprain, a Latissimus Dorsi strain, or an oblique injury doesn’t need seven months of structured throwing to return to sport.
They need a shorter, appropriately calibrated program that applies the same workload principles to a compressed timeline.
In our most recent paper in IJSPT, we expanded the framework to include four interval throwing programs of varying durations, covering the majority of injuries and surgeries a baseball pitcher might face:
- 6-Week Program – Designed for the short-duration returns. This is most commonly used in-season, where a player needs to return from a non-surgical injury as quickly as possible without losing more of the season. It can also be used for healthy athletes ramping up for the season. The program finishes with a chronic workload of 7.6 and stayed within the optimal ACWR range for the entire duration of the program – 100% of the time.
- 12-Week Program – A more conservative option for non-surgical injuries when there is more time available. Common applications include non-operative UCL injuries, lat strains, oblique injuries, and flexor-pronator strains. Also useful for healthy players wanting a more gradual preseason ramp-up. Finishes with a chronic workload of 7.9 and stayed within the optimal ACWR range 98% of the time.
- 5-Month Program – This is the program we now use for UCL repair with internal brace, an increasingly popular surgical option that offers outcomes equivalent to traditional reconstruction with a significantly shorter recovery timeline. Because the internal brace accelerates healing, athletes can typically begin this program around 10-12 weeks after surgery, allowing return to sport around seven to eight months post-op. Finishes with a chronic workload of 10.0 and stayed within the optimal ACWR range 95% of the time.
- 7-Month Program – The original long-term program for traditional Tommy John reconstruction, SLAP repairs, labral lesions, rotator cuff tears, and other significant surgeries requiring extended rehabilitation. Athletes typically begin around 20 weeks post-op, with return to competition near the 12-month mark. Finishes with a chronic workload of 10.8 and stayed within the optimal ACWR range 91% of the time.
As you can see, all four programs ended with appropriate chronic workloads to prepare them for competition while staying within the optimal ACWR range most of the time.
Even when the programs dipped outside the optimal range, they were just barely and immediately brought back into the optimal zone. This is typically when coming back from a deload week, and something we feel is clinically appropriate.
Together, these four programs cover the vast majority of baseball injuries. Clinicians can select the appropriate program based on the injury severity, the surgical procedure, the competitive calendar, and the individual athlete’s progression through rehabilitation.
What I’m particularly proud of is that all four programs are built on the same scientific framework. The same workload model. The same ACWR principles. The same modern throwing structure. We’re not guessing at these timelines; we’re reverse-engineering them from the biomechanical demands of competitive baseball pitching.
A Word on Radar and Velocity-Based Throwing Programs
I want to address something directly because I’m seeing it more often and have some concerns. Over the past few years, there has been a major trend toward using radar guns to monitor and progress interval throwing programs.
The idea is that velocity serves as a proxy for intensity. Hit a target velocity, and you’re cleared to progress. It sounds modern and objective, but the data tells a different story.
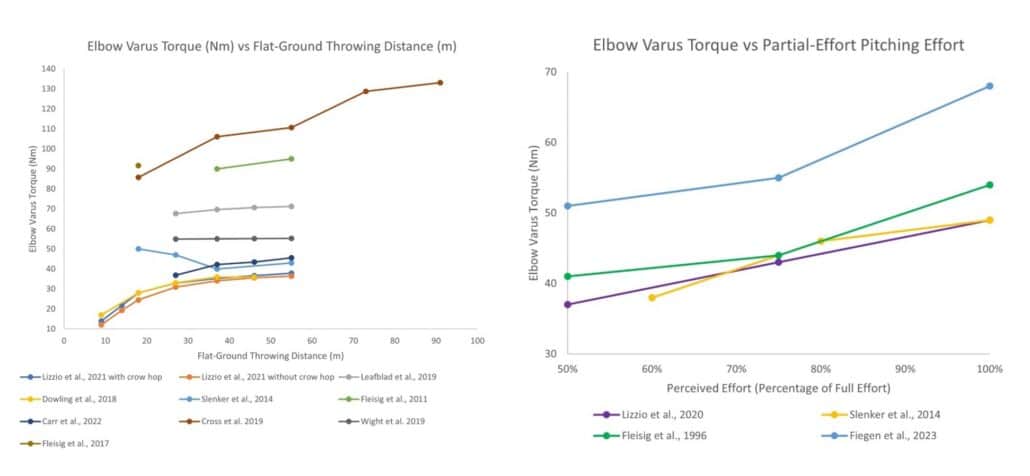
Here’s the problem: velocity and elbow varus torque do not correlate as well as distance and torque.
Research has consistently shown this. A study by Leafblad et al. found that as throwing distance increased during long-toss, velocity increased significantly, but elbow torque did not follow the same pattern.

Melugin et al. showed that during long-toss at 120 feet, pitchers throwing at 50% perceived effort produced 78% of maximum velocity but 87% of maximum elbow torque. At 75% effort, that jumps to 86% velocity and 93% torque. The relationship between effort and torque is non-linear and inconsistent, which makes velocity a poor and potentially dangerous proxy for the actual stress on the UCL.
Velocity-based programs have another practical problem: they are frequently used to set minimum intensity thresholds rather than maximum limits. What was once a tool to prevent throwing too hard has become a way to push harder and ramp faster.
I have recently seen alarming outcomes from athletes progressing through velocity-based programs. Stress reactions, bony fractures, and failed reconstructions that we almost never saw before. These are not isolated anecdotes. This is an alarming pattern that I am seeing.
Remember, the metric that matters when you are trying to protect healing tissue is torque – the mechanical stress directly applied to the UCL and surrounding structures.
Our programs are distance-based because distance has the strongest validated relationship with torque. And because they’re distance-based, they don’t require access to sensors, radar guns, or any technology whatsoever. That makes them accessible to everyone, from MLB rehab staff to a high school coach working with a kid in the backyard.
What This Means for You
I’ve been personally using and refining these programs for over 15 years. They work. They actually work extremely well. Our players progress through their ITPs with minimal concerns and return to pitching feeling like they are ready to compete.
The most important thing you can take from this work: we now have evidence that it is possible to return a pitcher to sport using a program that stays within the optimal ACWR range throughout the process.
That wasn’t true of the most popular programs in baseball medicine. It certainly isn’t true of the newer velocity-based programs.
It is true of these new programs. And because they are built on biomechanical workload data rather than clinical intuition, they can be objectively monitored and adjusted as technology improves and as individual athletes respond.
I believe that athletes who use these programs will return to sport with fewer setbacks during their throwing program, will be more competitive in their first season back, and will be at lower risk of reinjury. That has been our clinical experience over the past 15 years, and now we finally have the science to support it.
It’s been incredibly rewarding to finally publish them so that clinicians, coaches, and players everywhere can access and benefit from the same framework we’ve been using at Champion PT and Performance and in professional baseball settings with the players and teams I have worked with over the years.
Download my Interval Throwing Programs for Free

Now that the ITPs have been published, I want you to be able to freely use them with your athletes.
Fill out the form below, and I will send you copies of my interval throwing programs and our published journal articles.
I want you to be able to use them, but I would also love it if you read the articles so you have a full understanding of the science behind the development of these programs.



