
Total shoulder replacement surgery is being performed more and more each year. Our current patients were more active in sports in their youth, potentially increasing the chances of developing an arthritic shoulder. They also want to remain active as they age, potentially increasing the likelihood that they want to have a total shoulder arthroplasty surgery to allow them to remain active.
Over the years, the surgical technique for a total shoulder replacement has improved, though I’m not sure our rehabilitation approach has also improved. If our patients are younger and want to be more active after total shoulder replacement, then perhaps our rehabilitation programs should adjust based on their goals.
Rehabilitation Following Total Shoulder Replacement
Historically, a conservative approach was appropriate for many patients, as their needs and activity goals were less aggressive than many patients today. It was acceptable to have a moderate loss of range of motion in exchange for less pain in their shoulder.
Many surgeons continue to recommend a conservative approach to the restoration of range of motion following surgery.
It is true that one of the primary goals of the postoperative rehabilitation following total shoulder replacement is to protect the subscapularis. The subscapularis muscle is taken down to some extent during the surgical procedure and the integrity of this muscle has been correlated to the overall outcome of the procedure.
Other motions, such as behind the back and shoulder extension behind their body, also place the arthroplasty in a disadvantageous position and can lead to dislocation of the joint.
But even with these precautions, I am still an advocate of early range of motion, especially if you respect these restrictions.
Passive ROM and Active ROM are Not the Same
A recent report was recently published in Journal of Shoulder and Elbow Surgery that may actually be causing some confusion on when to start range of motion.
In the study, the authors compared a group of patients that began range of motion immediately versus a group that delayed 4 weeks. The authors reported that the immediate range of motion group gained more motion, restored it earlier, and also showed an earlier increase in functional outcome scores.
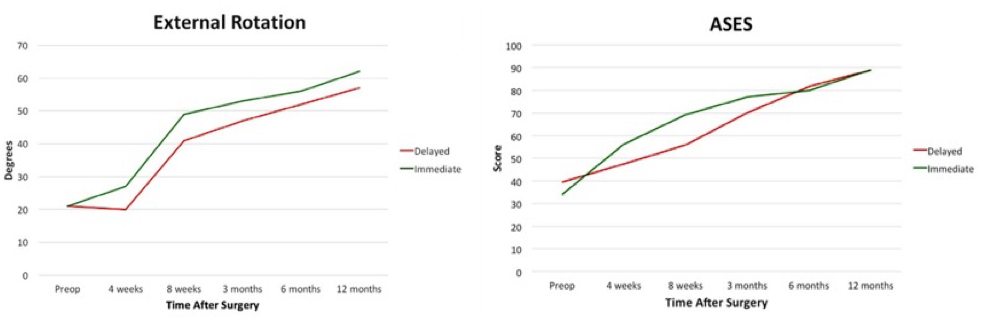
However, 96% of the patients that delayed range of motion showed healing of the lesser tuberosity osteotomy, while only 82% of the immediate range of motion group showed healing. Furthermore, functional outcomes scores 3 months and 1 year after surgery were similar between the groups.
This has led to many recommending a delay in range of motion. But…
When looking deeper at the methods, the authors chose to use the rope and pulley and stick elevation range of motion exercises. As we all know, these are not passive range of motion exercises, they are active assisted range of motion exercises.
There’s a big difference between passive and active range of motion exercises!
Previous EMG studies have shown the rotator cuff to be between 18-25% active and the deltoid to be between 21-43% active during these exercises. Not very passive. Conversely, passive range of motion exercises have been shown to be between 3-10% active.
This is a big difference. I believe passive range of motion is appropriate, as long as you respect the restrictions on restoring external rotation to protect the subscapularis and avoid behind the body and behind the back motions to protect the replacement.
Immediate Range of Motion Restores Function Faster
Since we all work with these patients after surgery, we know that they are always happier when they restore their motion sooner. And this increase in range of motion is likely related to the earlier improvement in functional outcome scores.
I think there is a middle ground of immediate, yet cautious, passive range of motion. Again, I want to reiterate, “passive” range of motion. Not active.
By focusing on this, I believe our patients will have much better outcomes.
Learn More About How I Evaluate and Treat the Shoulder

I’m pretty excited to announce I have revised my acclaimed online program teaching you exactly how I evaluate and treat the shoulder to now include a lesson on the arthritic shoulder! If you want to learn more about how I work with the arthritic shoulder, patients following total and reverse shoulder replacements, and everything else related to the shoulder, you’re going to want to take my online course.


