This week’s article is a guest post from Lenny Macrina. Lenny discusses a really important topic right now regarding the safe return to sport after ACL reconstruction. Are we returning people too fast? If you want to learn exactly how Lenny and I return people after ACL reconstruction be sure to check out our acclaimed online program on the Evaluation and Treatment of the Knee.
ACL reconstruction surgery continues to dominate the sports medicine and orthopaedic world. Research surrounding ACL surgery is abundant and I have written about it in previous posts on LennyMacrina.com and for Mike on his website. It’s an important topic because of the lack of general consensus on what’s the best way to assess return to play testing, never mind the relatively high failure rates.
For this post, I wanted to discuss the return to play testing after an ACL reconstruction to see what the literature says. I’m not going to lie, I don’t have a formal algorithm like some. I have people hop, skip and jump but don’t necessarily do a formal hop test.
I believe in slowly returning my athletes to their sport in a time that is safe. I carefully watch them move, advance their strength and power exercises and chat about how they feel about their knee.
With that, I wanted to do an extensive literature search to figure out what was the best way to truly test our athletes to determine their readiness.
Is there a best algorithm that will decrease retear rates? If so, why are we not using it for injury reduction programs…or are we?
Risks for ACL Reconstruction Failure
The risk of a second ACL injury in a young, active individual is high after a previous ACL reconstruction and return to sport.
Paterno and his group reported 23.5% of young, active patients suffered a second ACL injury in the first 12 months after RTS following ACLR.
Another study by Paterno and his colleagues showed 37.5% suffered a non-contact retear within 24 months after the initial reconstruction.
Surprisingly enough, this group also reported that 29.5% of young, active athletes who returned to cutting and pivoting sports after an ACL reconstruction suffered a second ACL injury 24 months after return to their sport.
A recent review by Wiggins et al showed that young, active athletes are at greater risk to suffer another ACL injury after ACL reconstruction and return to sport compared with uninjured adolescents.
With retear rates so high, there has to be a better strategy to get our athletes back to their sport safely.
ACL and Kinesiophobia
We know the mental component involving fear of movement/reinjury, or kinesiophobia, is often the last to come back for the athlete. A good majority of patients have some form of kinesiophobia after an ACL reconstruction and we need to be able to address that too. Numerous studies have shown this and it definitely needs to be understood and addressed as the program is progressed. Here’s another one for you to check out.
Those are just a couple of articles that discuss the self-reported fear that is involved in an athlete’s head. My pubmed search gave me 36 total articles that you may want to check out here.
There’s no denying the power of the mind when a return to play decision has to be made. I want them feeling as strong and confident as possible. It takes time and the days of trying to return someone back in 4-6 months seems to be a thing of the past. I did it.
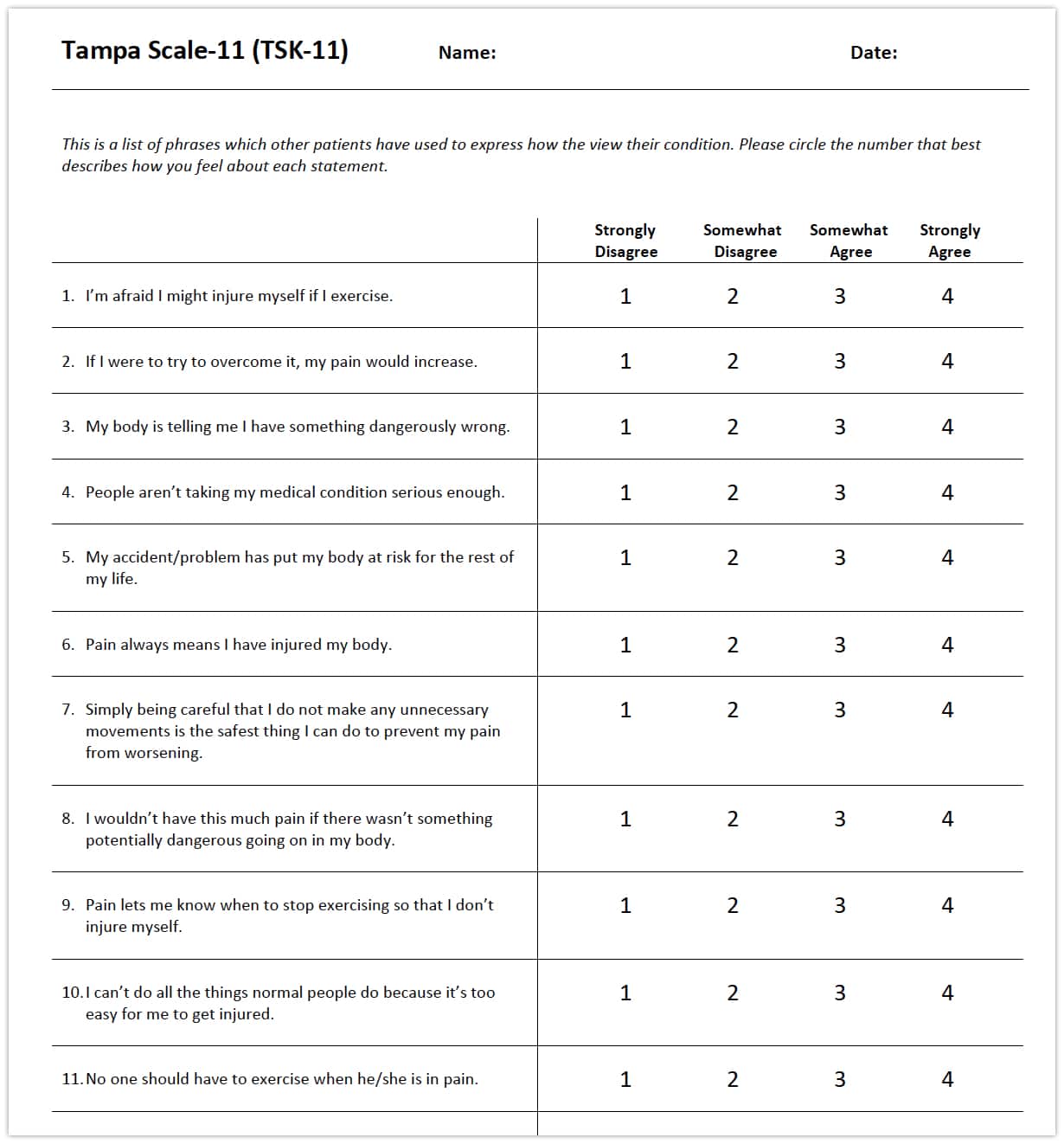
Some self-reported outcome measurements that are commonly used are the TSK-11, known as the Tampa Scale for KInesiophobia. This is a shortened version of the original TSK-17 that was published previously.
Another questionnaire that can be use is the ACL-RSI or the Return to Sport after Injury Scale. It is used to assess psychological impact that may be in the athlete’s head. The goal of the questionnaire is to the athlete’s emotion, confidence and self-risk appraisal.
There are many other tools out there that can gauge a patient’s knee function such as the IKDC, KOOS, VAS scale, Lysholm, Tegner, and the Cincinnati Knee Scoring scale. I just wanted to add those in as an informational thing but they don’t necessarily measure the psychological component ad readiness for return to play.
Slow and Steady ACL Rehabilitation
I’ve gotten high school seniors back to their sport quickly and bragged about it. Despite their isokinetic test being marginally ok, the docs would clear them because of other circumstances. It’s the last game of the season or it’s their senior year or they made the playoffs and the team ‘needs them.’
It seems as if the literature supports some form of formal testing but there is no clear answer, in my opinion.
The tests that many currently utilize in the clinic have just never felt right to me. I’m not sure we can simply do some hop tests or a step down test and have enough information to decide on whether an athlete is ready to return to their sport. Both tests are in the sagittal plane and don’t account for fatigue or other planes of movements such as the frontal plane (side to side) or transverse plane (rotational motions.)
Never mind that when we are comparing the involved leg to the uninvolved leg during functional testing to determine limb symmetry index (LSI), are we inherently flawed? Does the strength and proprioception of the uninvolved leg diminish months after the ACL reconstruction which makes our battery of tests invalid by inflating the LSI?
Rethinking the Way We Determine Return to Play After ACL Surgery
Delaware researchers seem to think that the LSI can overestimate knee function after an ACL surgery. They have shown that doing baseline functional tests soon after the ACL tear gives a better estimate of the body’s strength and functional output.
So if we’re using the uninvolved leg as the comparison leg and it has undergone strength and proprioceptive changes during the 6-12 months of rehab, are we flawed from the start and our LSI testing is invalid and over-estimates an athlete’s return to play?
Maybe that’s one reason why our retear rates are so high.
Physical Therapy Is Not Good at Advanced Stage Rehab
Never mind the pink elephant in the room… many PT’s are poor at prescribing higher level exercises. We just don’t see people past 8-12 weeks after surgery because of insurance visit limitations. We don’t have experience or the access to these patients once they’re discharged from PT.
It’s at this point that the real strength, power, endurance and agility activities really take shape. Unfortunately, most patients are on their own or working with other professionals. It is key that we maintain our relationships with other fitness professionals so we can influence and guide the later-stage rehab process.
But we often don’t, sadly.
It’s a long process, longer than we think and longer than the patient wants it to be.
Should We Delay Return to Sport Longer Than 12 Months?
This article talks about how the rehab is multifactorial and can often take 1-2 years to feel comfortable enough.
Even renowned ACL researcher Tim Hewett, known for his injury reduction programs, has advocated for a 2 year return to sport in one of his latest papers.
Most are not functionally ready to return to their sport even though they are cleared by their surgeon. It seems as if time is the number one decision maker and not necessarily functional tests of strength power and endurance.
This paper showed that at 6 months, 2 patients (3.2%) passed all criteria. At 9 months, seven patients (11.3%) passed all RTS criteria. Patients improved in all RTS criteria over time except for the IKDC score. Twenty-nine patients (46.8%) did not pass the strength criterion at 60°/s at 9 months after ACL reconstruction.
While this research paper looked at younger athletes cleared for sports participation After an ACL Reconstruction. Only 13.9% of the participants passed all of the criteria (IKDC, quadriceps and hamstring strength limb symmetry index (LSI), and single-leg hop test) 1 year after surgery
This study looked to assess the changes over time in patients tested at 6 months and 9 months after ACL reconstruction. At 6 months, only 2 patients (3.2%) passed all criteria. At 9 months, 7 patients (11.3%) passed all criteria.
What if they had a previous ACL tear and then they subsequently tear the contralateral side? What does the PT use for an index?
A study by the Zwolski group that the use of LSI’s during strength and performance tests may not be an appropriate means of identifying residual deficits in female patients after bilateral ACL reconstruction. They also concluded that “a better indicator of strength performance in this population may need to include a comparison of strength performance values to the normative values of healthy controls.”
There seems to be a persistent issue with getting the quadriceps muscle to return in our athletes. Despite our efforts, there seems to be a neuromuscular component that requires time and persistence.
This study showed that in patients an average of 7.5 months out of surgery demonstrated nearly a 30% weakness. They said diminished motor neuron recruitment or decreased motor-unit–firing frequency was likely contributing to reduced isometric quadriceps strength and interlimb asymmetries.
Another study looked to compare adolescent athletes ages 15-20 years old with adults ages of 21-30 years old. At the 8-month follow-up, 29% of the patients, in both age groups, who had returned to sport had recovered their muscle function in all 5 tests of muscle function (unilateral vertical hop; unilateral hop for distance; and unilateral side hop, isometric quad at 60° and knee flexion at 30°.) At the 12-month follow-up, the results were 20% for the adolescents and 28% for the adult patients.
Again, a large strength deficit at 12 months post-surgery despite our objective testing.
Never mind that most of these studies lum everyone together and don’t account for graft differences. In my opinion, we need to consider graft type as another variable that could contribute to retear rates and return to sport testing. I talked about graft selection in this blog post.
How Do We Determine When Safe to Return to Sports?
That’s the million dollar question. There are a few common ways that we can determine when it is safe to return to sports after ACL reconstruction.
Isokinetic Testing
Isokinetic testing has been used for many years and seems to be valid and reliable. Although this recent systematic review in BJSM stated that isokinetic strength measures have not been validated as useful predictors of successful RTS.
Oh great, now what?
Don’t forget, back in 1994 Kevin Wilk and his group looked to determine if a correlation exists between three commonly performed clinical tests: isokinetic isolated knee concentric muscular testing, the single-leg hop test, and the subjective knee score in anterior cruciate ligament reconstructed knees. They noted a positive correlation was noted between isokinetic knee extension peak torque (180, 300 degrees/sec) and subjective knee scores, and the three hop tests (p < 0.001).
The problem lies with many clinics having limited access or just don’t use them anymore.
Because of that, we’ve had to adjust our thinking and use ground based testing such as hop tests, isometric strength testing and agility tests.
The research says that “athletes who did not meet the discharge criteria before returning to professional sport had a 4x greater risk of sustaining an ACL graft rupture compared with those who met all 6 RTS criteria (isokinetic strength testing at 60°, 180° and 300°/s, a running t-test, single hop, triple hop and triple crossover hop tests.) In addition, hamstring to quadriceps strength ratio deficits were associated with an increased risk of an ACL graft rupture.
This study says that the single hop for distance and ACL-RSI were found to be the strongest predictive parameters, assessing both the objective functional and the subjective psychological aspects of returning to sport. Both tests may help to identify patients at risk of not returning to pre-injury sport.
Hand-Held Isometric Strength Testing
This is another test that is commonly used in return to sport testing after an ACL. I think it could be used but it gives limited information and can be painful if not done correctly. The painful response has been shown to statistically influence outcomes and needs to be modified to prevent alterations in true quadriceps force generation.
Also, the measurements using a hand held dynamometer are often lower than what can be obtained with an isokinetic device, as seen in this study.
I know many use hand-held dynamometry but I just can’t see its value as a return to sport test that is valid.
There are just too many questions about where to put the device to minimize pain while kicking. Also, at what angle do we place the knee to best isolate the quadriceps? Ninety degrees or 60 degrees of flexion? Research seems to look at both methods.
Plus, does a concentric, isometric contraction REALLY give us the information that we truly need to make an informed decision or have we sought a cheaper alternative to isokinetics and embraced it. We PT’s are suckers for the easiest way to diagnose, treat and test and often miss the big picture.
Research can guide us but common sense and experience must play some role as well.
Hop Tests to Determine Return to Play
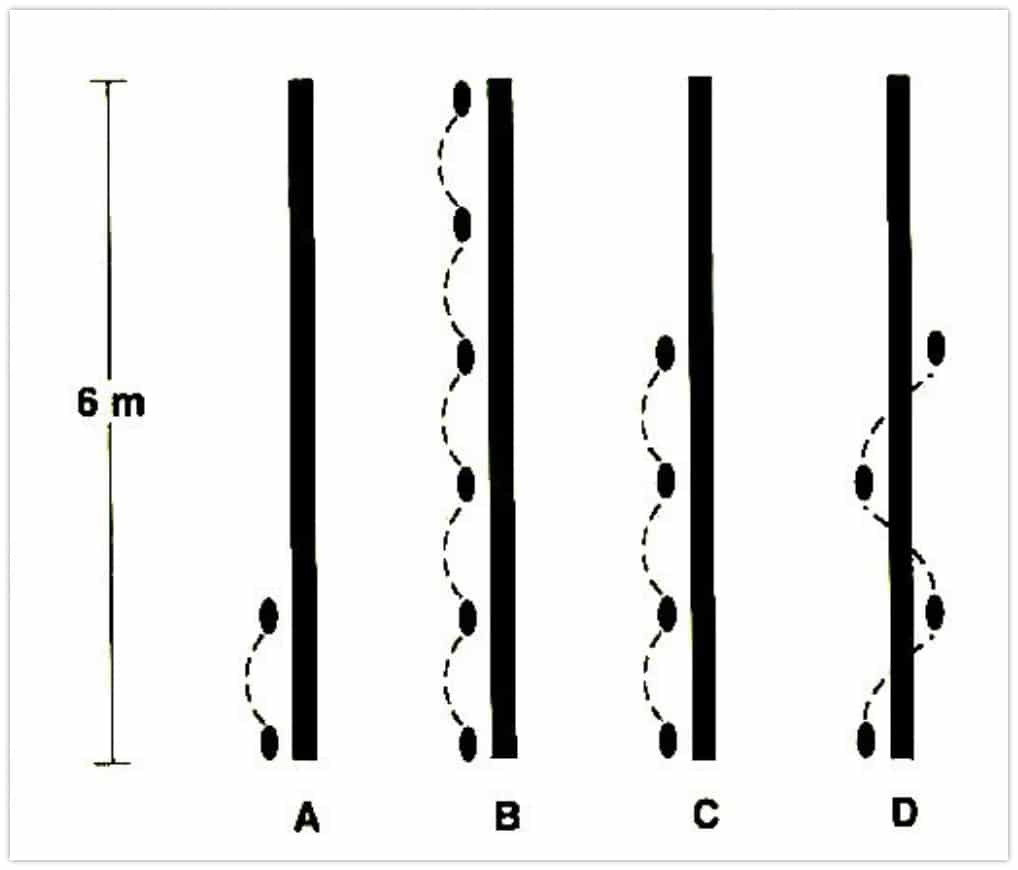
Hope tests are often utilized by rehabilitation specialists to determine an athlete’s ability to generate and dissipate a force when compared to their contralateral knee. As far as I can see, Noyes was one of the 1st to talk about hop tests in the literature in 1991.
Four common tests are utilized and reported in the literature. They include single leg hop for distance, triple hop for distance, crossover hop for distance and 6-meter time hop. The general rule is to obtain an LSI ≥ 90% compared to the reference limb.
As usual, both limbs are tested and the uninvolved limb is used as the reference, which we mentioned previously as an inherent potential flaw (the Delaware study.)
Using these tests can help the rehab specialist reduce ACL re-tears as noted in this study from BJSM in 2016. They showed reinjury rates were “significantly reduced by 51% for each month RTS was delayed until 9 months after surgery, after which no further risk reduction was observed.”
Furthermore, 38.2% of those who failed RTS criteria involving hop tests and quad strength symmetry within 10% suffered re-injuries versus 5.6% of those who passed all of the testing criteria.
Closing Thoughts on ACL Return to Sport Testing
My research has confounded my thoughts even more and added to the questions. It seems as if there is no clear way to determine readiness to return to sport after an ACL. Our testing seems somewhat flawed and despite our efforts, ACL retear rates are too high.
To simply say it comes down to strength is not enough. We’re so focused on quadriceps strength that we’re missing the big picture. Of course the quadriceps are highly important, bt don’t forget about hamstring:quadriceps ratios, gluteus strength, force attenuation, and fatigue-state rehab.
Never mind there’s the mental component and the ability to attenuate forces in game situations. These are things we cannot truly test.
We’re missing something but it does seem that the time-based scenario may be an option to consider, meaning they need to stay out of their sport for at least 9 months, and ideally 12-24 months, or as long as they are continually doing their progressive strength training.
I think therein lies the answer. As physical therapists, we don’t do a very good job at advanced strength training and periodization. We can learn a lot from our fellow strength coaches. Plus the fact that the athlete is all too eager to return to their sport without fully understanding the consequences.
Despite all of our testing, we continue to show poor outcomes even 12+ months after reconstruction. I can’t blame the tests, right? It’s the preparation for the tests that seems to be lacking.
What do you do to test your athletes when they’re considering a return to their sport?
Learn How We Evaluate and Treat the Knee

For those interested in learning more about how Lenny and I evaluate and treat the knee, we have an amazingly comprehensive course that covers everything you need to know to master the knee. Our detailed examination process, all our treatment progressions, and detailed information on nonoperative and postoperative treatment of ACL, patellofemoral, meniscus, articular cartilage, osteoarthritis injuries, and so much more.