
 A SLAP tear is an injury to the superior part of the labrum in the shoulder. The term SLAP stands for Superior Labral tear Anterior to Posterior. This is a very common diagnosis for shoulder injuries. There many different variations of SLAP tears, which have different levels of severity and treatment strategies. In the past, surgeons would want to operate on all SLAP tears but we have learned that some do well without surgery. In fact, some SLAP tears aren’t even worrisome .
A SLAP tear is an injury to the superior part of the labrum in the shoulder. The term SLAP stands for Superior Labral tear Anterior to Posterior. This is a very common diagnosis for shoulder injuries. There many different variations of SLAP tears, which have different levels of severity and treatment strategies. In the past, surgeons would want to operate on all SLAP tears but we have learned that some do well without surgery. In fact, some SLAP tears aren’t even worrisome .
Understanding how a SLAP lesion occurs and what exactly is happening pathologically is extremely important to diagnose and treat these shoulder injuries appropriately.
- Part 1: Classification of SLAP Lesions (You are here)
- Part 2: Mechanism of SLAP injuries
- Part 3: Special Tests for SLAP Lesions
- Part 4: How to Choose Which SLAP Test to Perform
Classification of SLAP Lesions
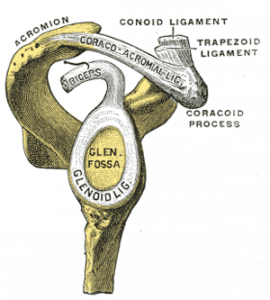
As you can see in the figure, the long head of the biceps tendon inserts directly into the superior labrum. There are several variations of injuries that can occur to the superior labrum where the biceps anchor attaches.
Following a retrospective review of 700 shoulder arthroscopies, Snyder et al: Arthroscopy 1990, identified 4 types of superior labrum lesions involving the biceps anchor. Collectively they termed these SLAP lesions, in reference to their anatomic location: Superior Labrum extending from Anterior to Posterior. This was the original definition but as we continue to learn more about SLAP tears, they certainly do not always extend from anterior to posterior. But, the most important concept to know is that a SLAP lesion is an injury to the superior labrum near the attachment of the biceps anchor.
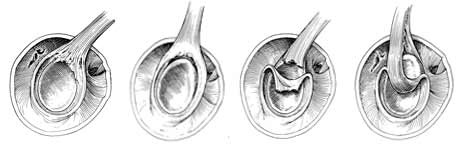
Type I SLAP Lesions
Type I SLAP lesions were described as being indicative of isolated fraying of the superior labrum with a firm attachment of the labrum to the glenoid. These lesions are typically degenerative in nature. At this time, it is currently believed that the majority of the active population may have a Type I SLAP lesion and this is often not even considered pathological by many surgeons.
Type II SLAP Lesions
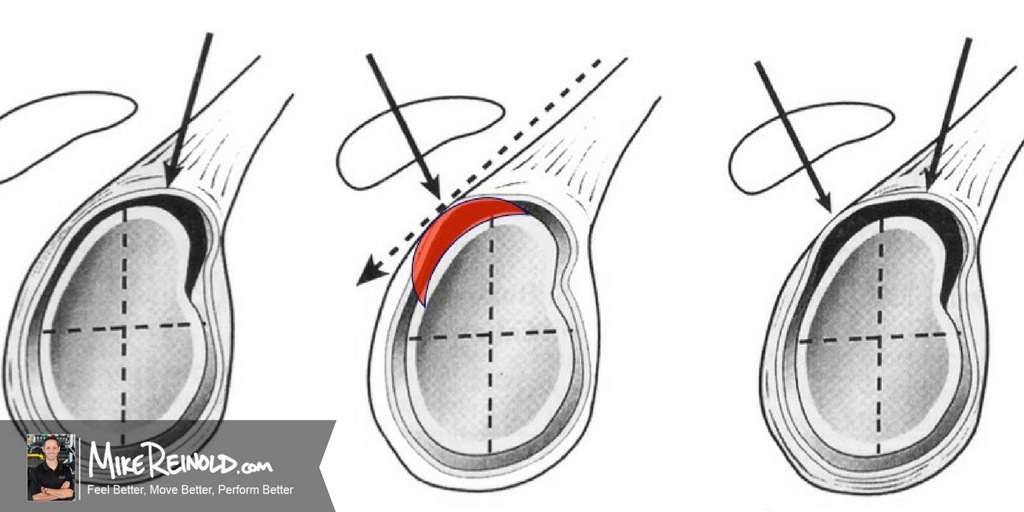
Type II SLAP lesions are characterized by a detachment of the superior labrum and the origin of the tendon of the long head of the biceps brachii from the glenoid resulting in instability of the biceps-labral anchor. These is the most common type of SLAP tear. When we receive a script from a surgeon to treat a “SLAP repair” he or she is more than likely talking about a Type II SLAP and surgery to re-attach the labrum and biceps anchor.
Three distinct sub-categories of type II SLAP lesions have been further identified by Morgan et al: Arthroscopy ’90. They reported that in a series of 102 patients undergoing arthroscopic evaluation 37% presented with an anterosuperior lesion, 31% with a posterosuperior lesion, and 31% exhibited a combined anterior and superior lesion.
These findings are consistent with my clinical observations of patients. Different types of patients and mechanisms of injuries will result in slightly different Type II lesions. For example, the majority of overhead athletes present with posterosuperior lesions while individuals who have traumatic SLAP lesions typically present with anterosuperior lesions. These variations are important when selecting which special tests to perform based on the patient’s history and mechanism of injury.
Type III SLAP Lesions
Type III SLAP lesions are characterized by a bucket-handle tear of the labrum with an intact biceps insertion. The labrum tears and flips into the joint similar to a meniscus. The important concept here is that the biceps anchor is attached, unlike a Type II.
Type IV SLAP Lesions
Type IV SLAP lesions have a bucket-handle tear of the labrum that extends into the biceps tendon. In this lesion, instability of the biceps-labrum anchor is also present, similar to that seen in the type II SLAP lesion. This is basically a combination of a Type II and III lesion.
- Type V SLAP lesions are characterized by the presence of a Bankart lesion of the anterior capsule that extends into the anterior superior labrum.
- Type VI SLAP lesion involve a disruption of the biceps tendon anchor with an anterior or posterior superior labral flap tear.
- Type VII SLAP lesions are described as the extension of a SLAP lesion anteriorly to involve the area inferior to the middle glenohumeral ligament.
These 3 types typically involve a concomitant pathology in conjunction with a SLAP lesion. Although they provided further classification, this terminology has not caught on and is not frequently used. For example, most people will refer to a Type V SLAP as a Type II SLAP with a concomitant Bankart lesion.
Since then there have been even more classification types described in the literature, up to at least 10 that I know of, but don’t worry, nobody really uses them.
Top 5 things you need to know about classifying SLAP lesions
Here’s all you need to know about classifying SLAP tears:
- Just worry about Type I-IV SLAP lesions and realize that any classification system above Type IV just means that there was a concomitant injury in addition to the SLAP tear.
- You can break down and group Type I and Type III lesions together. Both involved degeneration of the labrum but the biceps anchor is attached. Thus, these are not unstable SLAP lesions and are not surgically repaired. This makes surgery (just a simple debridement) and physical therapy easier.
- You can also break down and group Type II and Type IV lesions together. Both involve a detached biceps anchor and require surgery to stabilize the biceps anchor. Type IV SLAP tears are much more uncommon and will involve the repair and a debridement of the bucket handle tear.
- Type II lesions are by far the most common that you will see in the clinic and are almost always what a surgeon is referring to when speaking of a “SLAP repair.” That being said, we are seeing trends towards NOT repairing SLAP II lesions, as they may be more common than once expected. This is especially true in overhead athletes.
- We all may have a Type I lesion, it is basically just fraying and degeneration of the labrum.
Learn Exactly How I Evaluate and Treat the Shoulder
If you want to learn even more about the shoulder, my online course at will teach you exactly how I evaluate and treat the shoulder. It is packed with tons of educational content that will help you master the shoulder, including detailed information on the clinical examination and treatment of SLAP tears.


