
Today’s article is from my co-owner of Champion PT and Performance and co-author of OnlineKneeSeminar.com, Lenny Macrina. Lenny does a great job discussing and comparing the different options when it comes to graft choice for ACL reconstruction.
Tearing an ACL can be a devastating experience. Fortunately you are not alone as more than 250,000 people will tear their ACL in the United States and over 80% of people will have that tear reconstructed.
When the injury does occur, the person has some serious decisions to make including which graft to choose for the reconstruction. Often times, the person will leave that decision up to the orthopedic surgeon and blindly go with that decision.
All too often, the graft choice for that person may not be the best option for their age, goals and for their lifestyle, amongst many other things. Consideration for the current research should play a big role in this decision-making process on which graft to use for ACL reconstruction.
So, what graft choices are out there and why may one be better than another one?
Well, as I normally say ‘it often depends,’ but I usually coach my clients and start with the gold standard, consider the pros and cons, then move onto the next best option.
ACL Reconstruction Graft Choices
What are the options and why choose one over the other? First, I want to clarify the difference between “autograft” and “allograft.” Autograft means using your own tissue. Allograft means using tissue from a cadaver.
The most common choices available are:
- Patellar tendon autograft
- Hamstring autograft
- Quadriceps tendon autograft
- Patella tendon allograft
Let’s look at some of the research behind each ACL graft choice.
Patella Tendon Autograft
To me, the gold standard of ACL reconstruction is the patella tendon autograft and should be considered for most people in their teens, 20’s and for many in their 30’s or 40’s.
It is believed that the bone-patella tendon-bone graft has a stronger fixation because of the bone plugs that can incorporate into the femoral and tibial tunnels by 6-8 weeks after surgery.
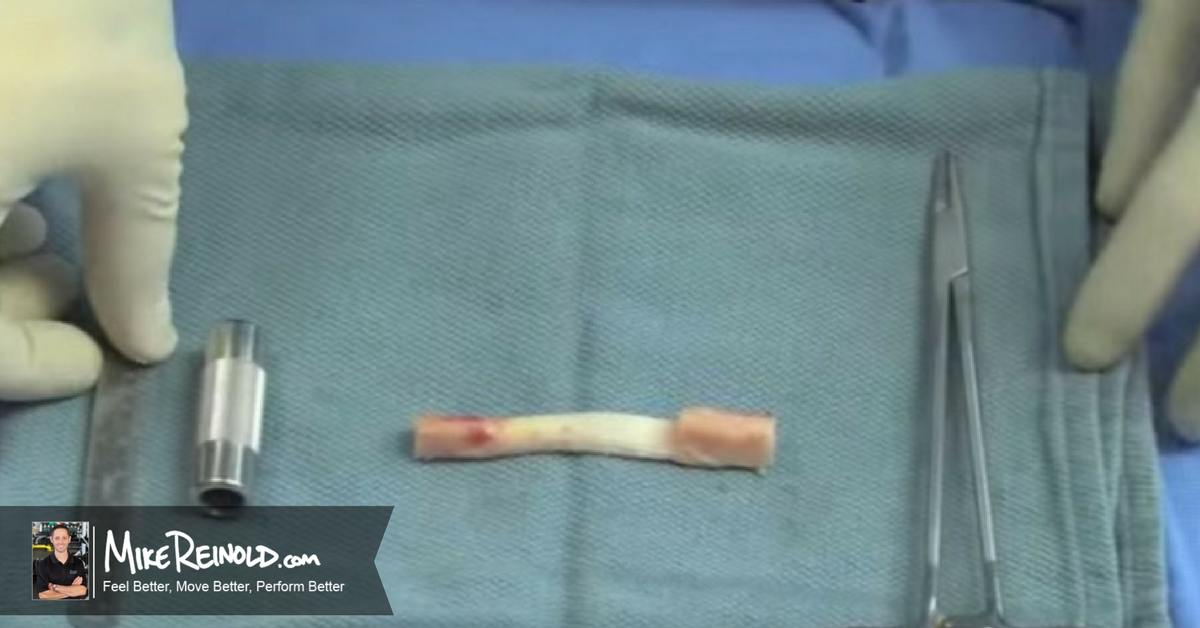
Better graft fixation may prevent stretching or excessive laxity that is often seen with hamstring autografts and allografts. A strong and stable graft is key when considering the long term stability of the knee joint, as seen in this video showing the harvesting of the graft and the reconstruction.
Numerous studies have shown that re-tear rates are also significantly lower in patients undergoing a reconstruction with a patella tendon versus a hamstring tendon autograft.
A Scandinavian study looking at nearly 46,000 reconstructions showed this as well as a Norwegian study looking at greater than 12,000 reconstructions. Furthermore a Danish study of nearly 14,000 reconstructions showed similar results.
Here in the US, a similar trend has been identified when looking at revision rates amongst the different graft choices. In this study out of over 21,000 reconstructions in California, patients under 21 years old with hamstring autografts had a 1.61 times higher risk of revision than did patients with patella tendon autografts. In patients less than 40 years old, those with allografts had a higher risk of revision than those with patellar tendon autografts.
A couple of disadvantages that are often reported after the surgery are an increase in general knee pain because of the soft tissue and bony dissection and anterior knee pain. This anterior knee pain may be more of a long term issue for some, especially while trying to kneel, because of the graft harvesting and scar that remains. To me, this is a small inconvenience but I always let my clients know of the potential long term kneeling limits. Usually not a big deal for most but you never know.
Some often say that it is more difficult to get a patient’s range of motion back, especially their hyperextension, if a patella tendon graft was used. I, personally have not seen this and have addressed this in a past article on 3 Ways to Avoid Loss of Motion After ACL Reconstruction.
I’ve actually had more difficult times getting hyperextension back in my hamstring autografts for some reason. They often feel that residual medial knee pain where the tendon was harvested and are reluctant to allow me to stretch them out into hyperextension.
Regardless, while anterior knee pain and range of motion restrictions are often cited as concerns, in my experience I feel these can be overcome with good postoperative rehabilitation.
Hamstring Tendon Autograft
The hamstring tendon autograft is another graft option for someone about to undergo an ACL reconstruction, as you can see in this video by Dr. Khalfayan:
https://www.youtube.com/watch?v=9EgRHfoleLc
I think it is too widely used currently and we need to further assess the outcomes and high risk of re-tear rate studies that I just presented.
Yeah, it may hurt less, and I stress MAY, but in my experience it is a graft that often presents a pretty big pain challenge. I’ve seen people in very comparable pain to a patella tendon graft because of the soft tissue dissection involved in the harvesting.
Think about a tendon shaver being poked under your skin high enough to clip the tendon from the muscle belly. No wonder hamstring grafts have a pretty significant bruising effect on the posterior aspect of their knees.
Ok, what about the famous: “But you can come back faster and progress rehab faster?”
I often hear this from patients who have done some research or have spoken to other health care practitioners but I completely disagree and actually progress people SLOWER with a hamstring autograft.
And here’s why…
The healing capacity for a hamstring autograft is believe to be inferior to the patella tendon graft. Remember the Ekdahl study from 2008 but there are others too.
I know many are in sheep, goats and dogs but that’s all we have to guide us right now. Until humans will volunteer their knees periodically through a study to get histological samples, then we have to rely on animal studies to guide our thoughts and progressions.
And don’t forget there is an increased risk of infection with a hamstring graft compared to a patella tendon autograft or allograft.
But good news, many say the hamstring will regenerate after being taken out although the strength deficits into knee flexion persist.
Because of this, I often progress my patients that have ACL reconstruction using a hamstring autograft much slower than those with patellar tendon autografts.
A slower healing potential that may lead to graft stretching and eventual failure, never mind the potential strength deficits that may persist and affect jumping/landing biomechanics due to the use of the hamstring.
Remember, the hamstrings line of pull will help limit anterior translation of the tibia and dynamically stabilize during running, jumping and cutting tasks. If we take 1-2 of those tendons out, how will that affect the athlete short term and long term as they return to their function/sport.
Maybe that’ another reason why re-tear rates are statistically higher in ACL’s reconstructed with a hamstring graft?
I definitely go slower with my female clients, as well, who are much more likely to tear their ACL’s, in general.
Remember, numerous studies like this, this, this, and this have shown females to land in a quadriceps dominant and valgus position, which may predispose them ACL rupture, amongst many other reasons.
So, why would we even consider a hamstring graft in an active female population and take away one for their main stabilizers. It’s almost like we’re promoting the quadriceps dominant position by “robbing Peter to pay Paul.”
For this reason, I almost always tell my female clients to highly consider a patella tendon autograft. Furthermore, I very rarely recommend a hamstring graft for most of my patients that ask.
I just feel like the risk of re-tear outweighs the POTENTIAL for increased anterior knee pain after surgery. They tend to agree, quite often.
Quadriceps Tendon Autograft
Another autologous graft option, which I feel is underutilized, is harvesting a quadriceps tendon autograft to reconstruct the ACL. Honestly, the more I researched this graft option, the more I consider this a truly viable choice.
This video give a great overview of graft harvesting for the quadriceps tendon:
Numerous studies have shown very good outcome compared to hamstring and patellar tendon autografts. I could make a pretty good sized list but have picked just a few to make my point. Like this one, this one, or this one.
Because of the size comparison and increased collagen present within the graft, the quadriceps tendon graft is definitely a graft with comparable strength qualities compared to the previous grafts mentioned.
This table, taken from the lectures at from my online course with Mike Reinold at OnlineKneeSeminar.com, summarized strength and strength to failure of the various graft choices.
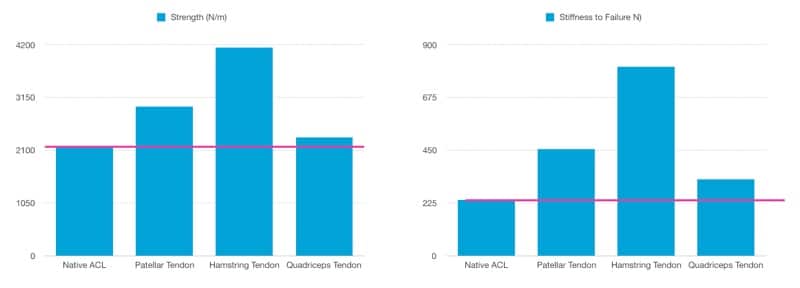
Biomechanically, the cross-sectional area of the quadriceps tendon was nearly twice that of the patellar tendon. Ultimate load to failure and stiffness were also significantly higher for the quadriceps tendon graft.
Well, maybe we consider a hamstring graft if the primary revision failed and we need a new graft option?
I still say maybe consider an ipsilateral quadriceps tendon before thinking about a hamstring tendon. This study showed revision ACL reconstruction using the quadriceps tendon graft showed clinical outcomes similar to those of the contralateral hamstrings graft in terms of knee stability and function.
But we said pain was less in hamstring grafts, right?
We’d rather have less pain so I can progress ROM and function quicker, no?
Well, maybe not, as this study showed comparing quadriceps to hamstring autografts. Supplementary analgesic drug was 38% higher in the hamstring group compared with the quadriceps tendon group.
Guess the hamstring option isn’t so painless!
Allograft Tissue
What about the ‘other’ graft choice that seems to be utilized a decent amount in the sports medicine and orthopedic world, the allograft.
Allograft tissue, or cadaver grafts, have recently become very popular in the United States for some reason, despite the numerous studies like this or this that show higher revision rates and graft stretching never mind the often under-reported cases of allografts being degraded by the body’s immune response.
I will say there is some research out there that is showing similar outcomes in allografts not chemically processed or irradiated when compared to autografts. But we are still learning.
This study looked at outcomes and revision rate after bone-patellar tendon-bone allograft versus autograft ACL reconstruction in patients aged 18 years or younger with closed physes. They determined there was no significant differences in function, activity, or satisfaction were found between allograft and autograft reconstructions BUT the allograft group had a failure rate 15 times greater than that in the autograft group, with all failures occurring within the first year after reconstruction.
I’ve spoken to surgeons who have reported almost no remnants of the previous allograft at the time of the revision surgery. It’s like the patient’s body completely rejected the graft.
That’s just a risk I almost never want to take.
I’d maybe consider an allograft for an older but active patient, say in their 50’s or 60’s but very rarely for an active person. I’d definitely not recommend an allograft to an athlete in their teens and 20’s although I have personally seen many kids present to me post- primary or revision surgery with an allograft reconstruction.
When I asked them why they chose it, they most often say: “it was recommended by the physician because I may be able to return to sports sooner and less pain.”
I could not disagree anymore and usually have to give them my dissertation on graft healing and the potential for graft rejection (as I mentioned previously).
Again, we think it takes several months longer for allograft tissue to incorporate itself compared to autograft tissue. There are very few reasons why someone should return their sport any quicker when the tissue is not fully incorporated, so why even consider it?
I very RARELY recommend an allograft for an ACL reconstruction. I frequently have to talk clients out of this option because the 1st thing they see or hear is there’s less pain. When they hear the whole story, they quickly realize an autograft seems to be the right choice.
Choosing the Right ACL Graft
Which autograft will depend on many factors but it seems like a patella tendon or quadriceps tendon may be the grafts of choice.
If you tore your ACL and are considering ACL reconstruction surgery, consider these factors when deciding which graft may be the most appropriate for you.
Learn How We Evaluate and Treat the Knee

For those interested in learning more about how Lenny and I evaluate and treat the knee, we have an amazingly comprehensive course that covers everything you need to know to master the knee. Our detailed examination process, all our treatment progressions, and detailed information on nonoperative and postoperative treatment of ACL, patellofemoral, meniscus, articular cartilage, osteoarthritis injuries, and so much more.


