
Shoulder impingement really is a pretty broad term that most of us likely take for granted. It has become such a junk term, such as “patellofemoral pain,” especially with physicians. It seems as if any pain originated from around the shoulder could be labeled as “shoulder impingement” for some reason, as if that diagnosis is helpful to determine the treatment process.
Unfortunately, There is no magical “shoulder impingement protocol” that you can pull out of your notebook and apply to a specific person. [Click to Tweet]
I wish it were the simple.
A thorough examination is still needed. Each person will likely present differently, which will require a variations on how you approach their rehabilitation.
But the real challenge when working with someone with shoulder impingement isn’t figuring out they have shoulder pain, that’s fairly obviously. It’s figuring out why they have shoulder pain.
Shoulder Impingement: 3 Keys to Assessment and Treatment
To make the treatment process a little more simple, there are three things that I typically consider to classify and differentiate shoulder impingement.
- Location of impingement
- Structures involved
- Cause of impingement
Each of these can significantly vary the treatment approach and how successful you are helping each person.
Location of Impingement
The first thing to consider when evaluating someone with shoulder impingement is the location of impingement. This is generally in reference to the side of the rotator cuff that the impingement is located, either the bursal side or articular side.
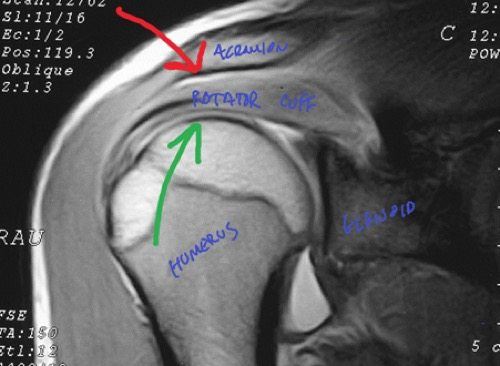
See the photo of a shoulder MRI above. The bursal side is the outside of the rotator cuff, shown with the red arrow. This is probably your “standard” subacromial impingement that everyone refers to when simply stating “shoulder impingement.” The green arrow shows the inside, or articular surface, of the rotator cuff. Impingement on this side is termed “internal impingement.”
The two are different in terms of cause, evaluation, and treatment, so this first distinction is important. More about these later when we get into the evaluation and treatment treatment.
Impinging Structures
To me, this is more for the bursal sided, or subacromial, impingement and refers to what structure the rotator cuff is impinging against. As you can see in the pictures below (both side views), your subacromial space is pretty small without a lot if room for error. In fact, there really isn’t a “space”, there are many structures running in this area including your rotator cuff and subacromial bursa.

You actually “impinge” every time you move your arm. Impingement itself is normal and happens in all of us, it is when it becomes excessive or abnormal that pathology occurs.
I try to differentiate between acromial and coracoacromial arch impingement, which can happen in combination or isolation. There are fairly similar in regard to assessment and treatment, but I would make a couple of mild modifications for coracoacromial impingement, which we will discuss below.
Cause of Impingement
The next thing to look at is the actual reason why the person is experiencing shoulder impingement. There are two main classifications of causes, that I refer to as “primary” or “secondary”shoulder impingement.
Primary impingement means that the impingement is the main problem with the person. A good example of this is someone that has impingement due to anatomical considerations, with a hooked tip of the acromion like this in the picture below. Many acromions are flat or curved, but some have a hook or even a spur attached to the tip (drawn in red):

Secondary impingement means that something is causing impingement, perhaps their activities, posture, lack of dynamic stability, or muscle imbalances are causing the humeral head to shift in it’s center of rotation and cause impingement. The most simply example of this is weakness of the rotator cuff.
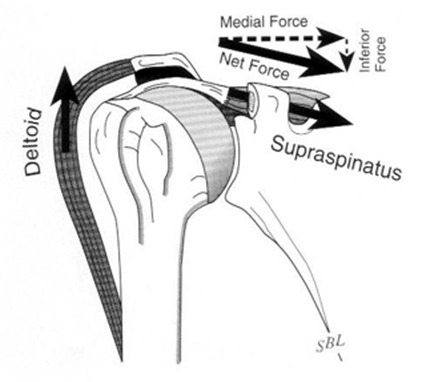
The rotator cuff and larger muscle groups, like the deltoid, work together to move your arm in space. The rotator cuff works to steer the ship by keeping the humeral head centered within the glenoid. The deltoid and larger muscles power the ship and move the arm.
Both muscles groups need to work together. If rotator cuff weakness is present, the cuff may lose it’s ability to keep the humeral head centered. In this scenario, the deltoid will overpower the cuff and cause the humeral head to migrate superiorly, thus impinging the cuff between the humeral head and the acromion:
Other common reasons for secondary impingement include mobility restrictions of the shoulder, scapula, and even thoracic spine. We see this a lot at Champion. In the person below, you can see that they do not have full overhead mobility, yet they are trying to overhead press and other activities in the gym, flaring up their shoulder.

If all we did with this person was treat the location of the pain in his anterior shoulder, our success will be limited. He’ll return to gym and start the process all over if we don’t restore this mobility restriction.
The funny thing about this is that people are almost never aware that they even have this limitation until you show them.
Differentiating Between the Types of Shoulder Impingement
In my online program on the Evidence Based Evaluation and Treatment of the Shoulder, I talk about different ways to assess shoulder impingement that may impact your rehab or training. There are specific tests to assess each type of impingement we discussed above.
The two most popular tests for shoulder impingement are the Neer test and the Hawkins test. In the Neer test (below left), the examiner stabilizes the scapula while passively elevating the shoulder, in effect jamming the humeral head into the acromion. In the Hawkins test (below right) the examiner elevates the arm to 90 degrees of abduction and forces the shoulder into internal rotation, grinding the cuff under the subacromial arch.

You can alter these tests slightly to see if they elicit different symptoms that would be more indicative to the coracoacromial arch type of subacromial impingement. This would involve the cuff impingement more anteriorly so the tests below attempt to simulate this area of vulnerability.
The Hawkins test (below left) can be modified and performed in a more horizontally adducted position. Another shoulder impingement test (below right) can be performed by asking the patient to grasp their opposite shoulder and to actively elevate the shoulder.

There is a good chance that many patients with subacromial impingement may be symptomatic with all of the above tests, but you may be able to detect the location of subacromial impingement (acromial versus coracoacromial arch) by watching for subtle changes in symptoms with the above four tests.
Internal impingement is a different beast.
This type of impingement, which is most commonly seen in overhead athletes, is typically the result of some hyperlaxity in the anterior direction. As the athlete comes into full external rotation, such as the position of baseball pitch, tennis serve, etc., the humeral head slides anterior slightly causing the undersurface of the cuff to impingement on the inside against the posterior-superior glenoid rim and labrum. This is what you hear of when baseball players have “partial thickness rotator cuff tears” the majority of time.

The test for this is simple and is exactly the same as an anterior apprehension test. The examiner externally rotates the arm at 90 degrees abduction and watches for symptoms. Unlike the shoulder instability patient, someone with internal impingement will not feel apprehension or anterior symptoms. Rather, they will have a very specific point of tenderness in the posterosuperior aspect of the shoulder (below left). Ween the examiner relocates the shoulder by giving a slight posterior glide of the humeral head, the posterosuperior pain diminishes (below right).

3 Keys to Treating Shoulder Impingement – How Does Treatment Vary?
There are three main keys from the above information that you can use to alter your treatment and training programs based on the type of impingement exhibited:
Subacromial Impingement Treatment
To properly treat, you should differentiate between acromial and coracoacromial impingement. Treatment is essentially the same between these two types of subacromial impingement, however, with coracoacromial arch impingement, you need to be cautious with horizontal adduction movements and stretching. This is unfortunate as the posterior soft tissue typically needs to be stretched in these patients, but you can not work through a pinch with impingement!
A “pinch” is impingement of an inflamed structure!
Also, I would avoid elevation in the sagittal plane or horizontal adduction exercises.
Primary Versus Secondary Shoulder Impingement
This is an important one and often a source of frustration in young clinicians. If you are dealing with secondary impingement, you can treat the persons symptoms all you want, but they will come back if you do not address the route of the pathology!
I do treat their symptoms, that is why they have come to see me. I want to reduce inflammation. However, this should not be the primary focus if you want longer term success.
This is where a more global look at the patient, their posture, muscle imbalances, and movement dysfunction all come into play. Break through and see patients in this light and you will see much better outcomes.
A good discussion of the activities that are causing their symptoms may also shed some light on why they are having shoulder pain. Again, using the example above, if you don’t have full mobility and try to force the shoulder through this tightness you are going to likely cause some issues. This is especially true if you add speed, loading, and repetition to elevation, such as during many exercises.
Internal Impingement
One thing to realize with internal impingement is that this is pretty much a secondary issue. It is going to occur with any cuff weakness, fatigue, or loss of the ability to dynamically stabilize. The athlete will show some hyperlaxity in this athletic “lay back” shoulder position. Treat the cuff weakness and it’s ability to dynamically stabilize to relieve the impingement. How to treat internal impingement is a huge topic that I cover in a webinar for my Inner Circle members.
Learn Exactly How I Evaluate and Treat the Shoulder
If you are interested in mastering your understanding of the shoulder, I have my acclaiming online program teaching you exactly how I evaluate and treat the shoulder at ShoulderSeminar.com!
The online program at takes you through an online 8-week program with new content added every week. You can learn at your own pace in the comfort of your own home. You’ll learn exactly how I approach:
 The evaluation of the shoulder
The evaluation of the shoulder- Selecting exercises for the shoulder
- Manual resistance and dynamic stabilization drills for the shoulder
- Nonoperative and postoperative rehabilitation
- Rotator cuff injuries
- Shoulder instability
- SLAP lesions
- The stiff shoulder
- Manual therapy for the shoulder
The program offers 21 CEU hours for the NATA and APTA of MA and 20 CEU hours through the NSCA.
Click below to learn more!



