Assessing overhead arm elevation is one of the many things I look for during my integrated movement assessment. This is a big part of the Champion Performance Specialist program. The information you gather on the person’s ability to perform such a basic task is often invaluable when designing someone’s rehab or training program.
I have a video below of an assessment I performed that I wanted to share. It’s an interesting case with a bunch of movement compensations. I thought it would be nice to outline my thought process
But first, let me give you a little history…
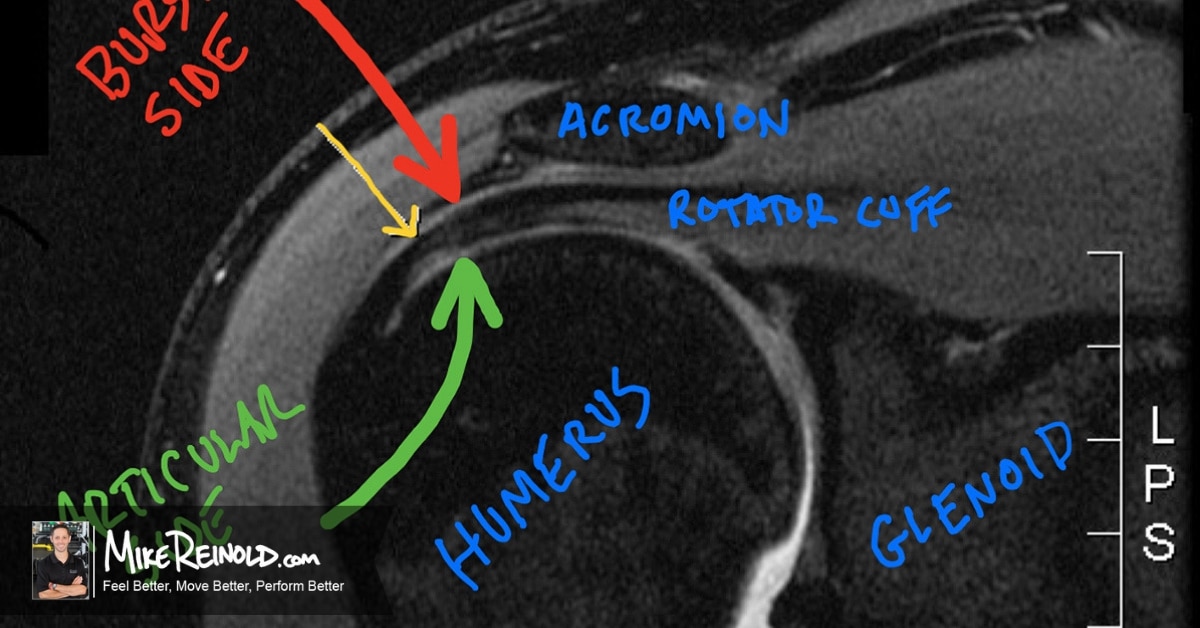
The patient is a competitor high school swimmer with insidious onset of bilateral generalized shoulder discomfort and fatigue in the pool after prolonged swimming. He had been seeing another clinician for soft tissue treatments in the past (hence the cupping marks. His laxity was mostly posterior in nature, but certainly multidirectional. The exam obviously reveals generalized laxity you would expect with a swimmer, however no significant structural pathology detected.
Here’s what I saw:
Pretty interesting, right? Scroll down to the comments section and let me know what you think!
Let’s dig into some of my thoughts.
Assessing Overhead Arm Elevation
- I would first comment and state that this is one quick video in a long series of assessments. I chose overhead elevation because it was simple and reproducible and showed a bunch of interesting things! I start my assessment off by simple asking them to raise their arms over head. That is it. No other instructions. I feel that it is important to assess how “they” want to move, not how “I” want them to move.

- A test like overhead elevation in the sagittal plane, such as in this video, assumes two thing: symmetry and neutrality. I don’t think either of these exist. So it is inherently flawed. Think about it, if his scapulae are off, then doesn’t that mean his glenoid is off? Then technically the “sagittal” plane is just in relation to the ground, not to his body.
- There is also a “chicken and the egg” concept here. Did his pain create the dysfunctional movement or vice versa? Unfortunately in retrospect we’ll never know. Taking this into consideration I don’t think it is fair to assume that anything we are seeing is the “cause” of his pain. Essentially it is all just the summation of where we are today.
- Many people often want to jump right in and label specific muscles, such as being “tight,” “long,” “short,” or “weak.” Remember all we know here is that he has a movement dysfunction. I think it is appropriate to suggest these may be true, but you will need to take the next step and assess these assumptions. I wouldn’t just jump in and treat based on assumptions.
- I should also comment on the marks on his back. One relevant, the other not so relevant. The circles are cupping marks. He is seeing another provider that performs this as part of his maintenance program while swimming in addition to massage etc, not for treatment of his symptoms. However, the horizontal marks on his low back are relevant. Those are stretch marks. More on this later…

Static Scapula Position
- I have commented on this before in my article on Myths of Scapula Exercises, but I don’t put a lot of emphasis on resting static scapular position. Realistically, the scapula sits on the ribs, so it’s resting static posture is likely more a reflexion of rib and thorax position that scapular position. I prefer to look at scapular dynamic movement quality.
- Interestingly, you can see his dynamic concentric control of his scapulae doesn’t seem as bad as you would think based on his static resting position, especially as he gets high into elevation:

The Head Wiggle and Scapula Wing
- The first thing that really stuck out to me was his head wiggle. I bet you missed it the first time! A very interesting movement pattern. In retrospect, you can find him shift his neck in this fashion quite a bit while observing him moving around and performing activities, even just talking to you sometimes. It is not limited to just overhead elevation in the sagittal plane.
- We can’t really separate this from his winging scapula, they go together. It sure looks like the head wiggles when the scapula wiggles.
- To me, this looks like the levator scapula pulling the head with a complete lack of opposition from the lower trapezius and serratus anterior. His head goes into side bend to the left and extension. This is the cervical responsibility of the levator. However, his scapula also shoots up into elevation and downward rotation. This is my biggest indicator that levator is the one acting. There could be more involved, like SCM, but I’m focusing on levator.
- There is obviously some winging and lack of opposition of the levator by the traps and serratus. This is really obvious on eccentric lower. He also does not have a painful arc during this movement. He is not shifting away from pain.

- So while the levator may be causing the head wiggle, it sure looks like the serratus and lower trap are not doing their job and creating the scapula wiggle.
- See how everything plays together?
The Elbow Wiggle
- Did you notice the elbow wiggle? I don’t think this is really an elbow issue. If you watch closely he keeps his hand in the same position. He essentially fixes his hand on an imaginary sagittal plane track. To me his shoulder and scapula want to move into adduction and internal rotation with the beginning of his scapula winging about to occur. I feel like his glenoid may be the one the is not stabilized. Since we have forced him to perform a strict overhead assessment in the sagittal plane, he is keeping his hand fixed and his elbow has to hyperextend to not allow his hand to horizontal adduct. Again, just shows some of the flaws of assessments like this.

- So while this may be glenohumeral instability, I think it is still just the scapula as it occurs during the eccentric lowering and he has almost no ability to control winging. And again, he does not have a painful arc.
- This really illustrates a general point that I tend to make about humans in general, but even more so on high level athletes. We are excellent at getting from point A to point B. It’s all about how we get there. Unfortunately the overhead elevation assessment uses an internal cue to “raise your hand up in front of you.” Perhaps it would be better to give an external cue like “reach up and touch the ceiling.”
Thoracolumbar Flexion
- So taking away all the interesting things happening from the scaps up, I also notice some interesting thoracolumbar compensations. Remember, this client is a swimmer, and a high level swimmer. Is it me or does his left latissimus look too small for a swimmer?
- I mentioned earlier the stretch marks on his lower back. When he tries to pull down with his arms with any resistance, his movement compensation was to go into a large amount of thoracolumbar flexion, which is a compensatory movement for the inability to extend his arms against resistance. His lumbar paraspinals show hypertrophy. So while this could be poor core control, I feel that may be too simplistic. He goes into thoracolumbar flexion with minimal resistance. Seems more compensatory rather than poor patterning. In the photos below, that is not just paraspinal hypertrophy, that is also flexion:

- In looking at the photos above, see how he moves into thoracolumbar flexion? These are fairly recent photos. Here are a couple of photos from two months prior. You can really see the thoracolumbar flexion compensation. But also notice the dramatic increase in body composition in 2 months. He put on 15 pounds of muscle mass in a 2-month program designed specifically for him:

- One thing I mentioned was that he feels symptoms with prolonged swimming. He actually fatigues out well before his fellow swimmers. Feels strong and swims well, then hits a wall quickly from 10-20 minutes in the pool, while everyone else is in there for 60-120 minutes without complaints. While he looks a lot better. There are still some muscles that are not coming back as expected, and he is still fatiguing out in the pool and feeling generalized symptoms.
- This really makes me question a nerve issue that is just not allowing proper muscle function, and/or the fact that he is essentially swimming with his accessory muscles like his teres major and deltoids. This is something we need to explore further.
Conclusion
Assessing overhead arm elevation is an important part of my overall movement assessment process. There are many compensations that I typically see, but most don’t present as complex as this video case study. I hope you enjoyed reading through my breakdown of how I assess overhead arm elevation and some of the things running through my mind!
Comment below if you think I missed anything!
Interested in learning my whole movement assessment system? It’s a part of my Champion Performance Specialist program, where you’ll learn our exact system of assessing movement, then optimizing and enhancing performance. It’s exactly what all the physical therapists and strength coaches follow at Champion when building our performance therapy and training programs.