
The October 2008 issue of the Journal of Strength and Conditioning has an impressive review article of the anatomy, function, assessment, and strengthening of the gluteus medius from a group of clinicians in New Zealand. The authors do a good job reviewing some of the basic anatomy and function of the muscle and relating this information to research reports looking at dysfunction and treatment of the muscle for several lower extremity injuries.
I think this is a great topic of discussion as the role of the gluteus medius in normal function and rehabilitation has been receiving attention lately as attention is being paid to strengthening and training the body in the frontal plane of motion and out of the sagittal plane.

The Role of the Gluteus Medius
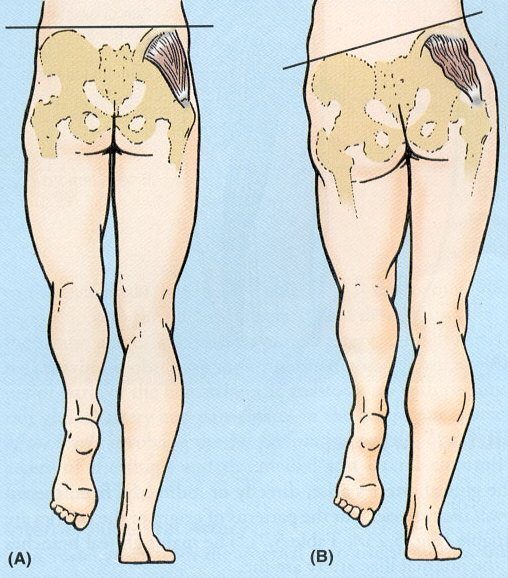
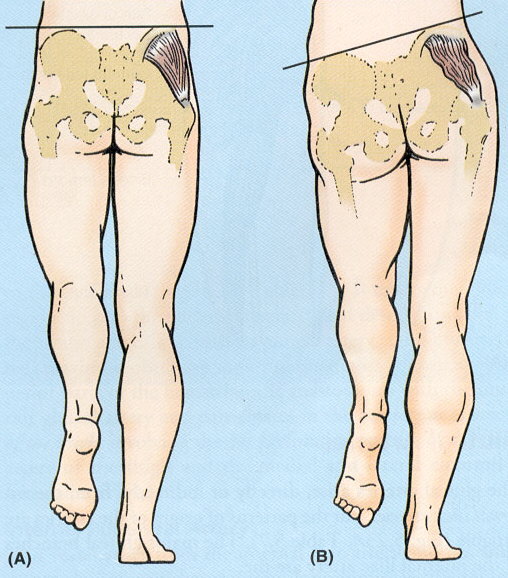
When you really break down the function of the gluteus medius, you see that it is far more valuable as a pelvis and lower extremity dynamic stabilizer than it is a pure hip abductor. This is apparent when looking at the mechanism of a Trendelenburg Gait. The role of the gluteus medius during activities such as walking and running is to dynamically stabilize the pelvis in a neutral position during single leg stance. As you can see in the photo below, weakness of the right gluteus medius will cause the left hip to drop when standing on the right limb. Conversely, athletic patients are often masters of compensation and may be able to keep the pelvis in neutral while the lower leg will adduct and internally rotate.

In addition, the role of the gluteus medius as an external rotator of the hip when the hip is in a position of flexion is also important to consider. These factors together are likely why dysfunction of this muscle is commonly found in several pathologies, such as iliotibial band, patellofemoral injuries, ACL, and ankle injuries.
Assessment of the Gluteus Medius
The authors describe several methods of evaluating the gluteus medius. These include:
- Standard manual muscle testing of hip abduction in sidelying. Because the gluteus medius also has an effect on other hip motions, I often recommend a full testing of hip flexion, abduction, ER, IR, and extension as well.
- Double- to single-leg stance test. Simply a test such as the photo above. The patient is instructed to stand on one limb and pelvis orientation is documented.
- The authors also recommend adding an upper body movement to the single-leg stance test. This will further challenge the patient, specifically the athletic patient. During this, the patient is instructed to balance on one limb while reaching the arms overhead and leaning away from the stance leg. This will move the patient’s center of gravity further away from the stance limb and require a greater amount of gluteus medius stabilization to avoid the dropped pelvis position.
- In addition to the above described, I would also recommend that patients should be observed during several functional activities, especially if a specific activity tends to exacerbate symptoms. This could include eccentric step-downs, front lunges, or even running and jumping activities for athletes. Watching the kinematics of the pelvis and lower body closely can be very beneficial. Personally, I often try to video tape these movements as well. For my athletes I have sophisticated camera systems but I also travel with a simple flip cam that I plug in to my laptop and quickly record and view back with my patients. I actually do not like the actual Flip cams, the angle of the lens is terrible. I actually use and really love the Creative Vado – check it out on Amazon. In addition to having a better wide angle lens, I can control the video quality. It is inexpensive, small, portable, plugs into my computer for charging, and shots great video. In just a few minutes I have a great quality video to watch with my patients. I try to take it a step further a draw on my videos and photos as well.

Treating the Gluteus Medius
While the beginning of the paper provides a brief, yet basic, review of the normal anatomy, function, and potential for injury implications of gluteus medius weakness, the strength of the paper lies in the later half that reviews the evidence behind some exercises designed to strengthen the gluteus medius.
The authors provide a thorough table that lists the many exercises described for gluteus medius strengthening. Most of these are basic recommendations, such as sidelying hip abduction straight leg raises and standing hip abduction. However, the authors combine the work and recommendations of three articles to develop a gradually progressive exercise program.
The progression is designed to gradually enhance motor control, endurance, and strength. The program is broken down into three phases:
- Phase I: Nonweightbearing and basic weightbearing exercises such as clam shell exercises, sidelying hip abduction, standing hip abduction, and basic single leg balance exercises. Criteria to progress to stage II is that the patient can hold their pelvis level during single leg stance for 30 seconds.
- Phase II: The second stage progresses the weight-bearing exercises and gradually progresses stability exercises by (a) translating the center of gravity horizontally via stepping and/or hopping exercises; (b) reducing the width of the base of support, (c) increasing the height of the center of gravity by elevating the arms and/or hand-held weights, or (d) performing the exercises on unstable surfaces.
- Phase III: The third stage is used for athletes and designed to prepare them for function, sport-specific movement patterns.
I agree with this progression but think that the authors are missing one key point regarding training of the gluteus medius. Because it is such a valuable component of dynamic pelvis and lower extremity stability. I also would encourage clinicians to also incorporate exercises designed to promote hip stability during normal sagittal plane movements such as squatting. To do this, I often just simply incorporate a piece of exercise tubing around the distal thigh (just higher than the knee) of the patient during exercises such as mini-squats, wall squats, and leg press. The patient is instructed to isometrically set the hips in a neutral position while performing the exercise. Cueing is often needed at first to be sure that the patient does not let their hips drip into adduction and internal rotation. I have found great success in this type of exercise as it required the hips to dynamically stabilize against a hip adduction/internal rotation moment during common functional activities.

There is also a section that reviews some of the available evidence behind choosing sets, repetitions, frequency and duration of rehabilitation programs. Overall, a great review of some of the basics regarding the gluteus medius and definitely a great starting point to develop a comprehensive rehabilitation or injury prevention program.
Check out my other post on an article reviewing more great information on gluteus medius exercises and gluteus maximus exercises.
Presswood L, Cronin J, Keogh J, Whatman C (2008). Gluteus Medius: Applied Anatomy, Dysfunction, Assessment, and Progressive Strengthening. Strength and Conditioning Journal, 30 (5), 41-53
Images from: Prevent Disease, UWO
Want to learn more about how to get the most out of the hips and glutes? I have two great inner circle webinars on My Top 5 Tweaks to Enhance Hip Exercises and How Pelvic Position Influences Lower Extremity Stretching. Click here to learn more about my Inner Circle and how you can gain access to these webinars and more for only $5.
![]()


{kind=link}
{kind=link}